Session Information
Session Type: Poster Session D
Session Time: 8:30AM-10:30AM
Background/Purpose: Hydroxychloroquine (HCQ) is an antimalarial drug used in the treatment of systemic lupus erythematous (SLE). There is limited data assessing cardiac toxicity as arrhythmias in association with HCQ exposure based on dose prescribed or pharmacy records and none relying on measured drug levels. Some of the risk factors associated with conduction abnormalities in the setting of hydroxychloroquine use include presence of chronic kidney disease, older age, underlying cardiomyopathy, and the use of concomitant prolonging QTc agents. In a retrospective study of 194 SLE patients on HCQ, the authors found that there was no significant difference in mean QTc based on HCQ use. Additionally, patients with CKD were more likely to have prolonged QTc when compared to those without CKD, but there was no significant difference in mean QTc based on HCQ use as well in this subset. Severe prolongation of QTc was rare in all groups and no episodes of serious tachyarrhythmia or Torsade de Pointes were observed. The purpose of this study is to determine the relationship between whole blood HCQ levels and QTc intervals on simultaneous EKG performed during a routine visit.
Methods: This prospective study was IRB approved and all patients provided consent. At the time of data lock, 84 patients fulfilled ACR/SLICC criteria for SLE. These patients were on HCQ for at least 3 months at doses used for standard of care treatment. Whole blood levels were drawn and EKGs were obtained during a routine outpatient faculty practice visit for patients consecutively seen between February 5 and May 10, 2021 with senior author. Statistical analyses was performed using one way ANOVA, Pearson’s correlation coefficient and t-test.
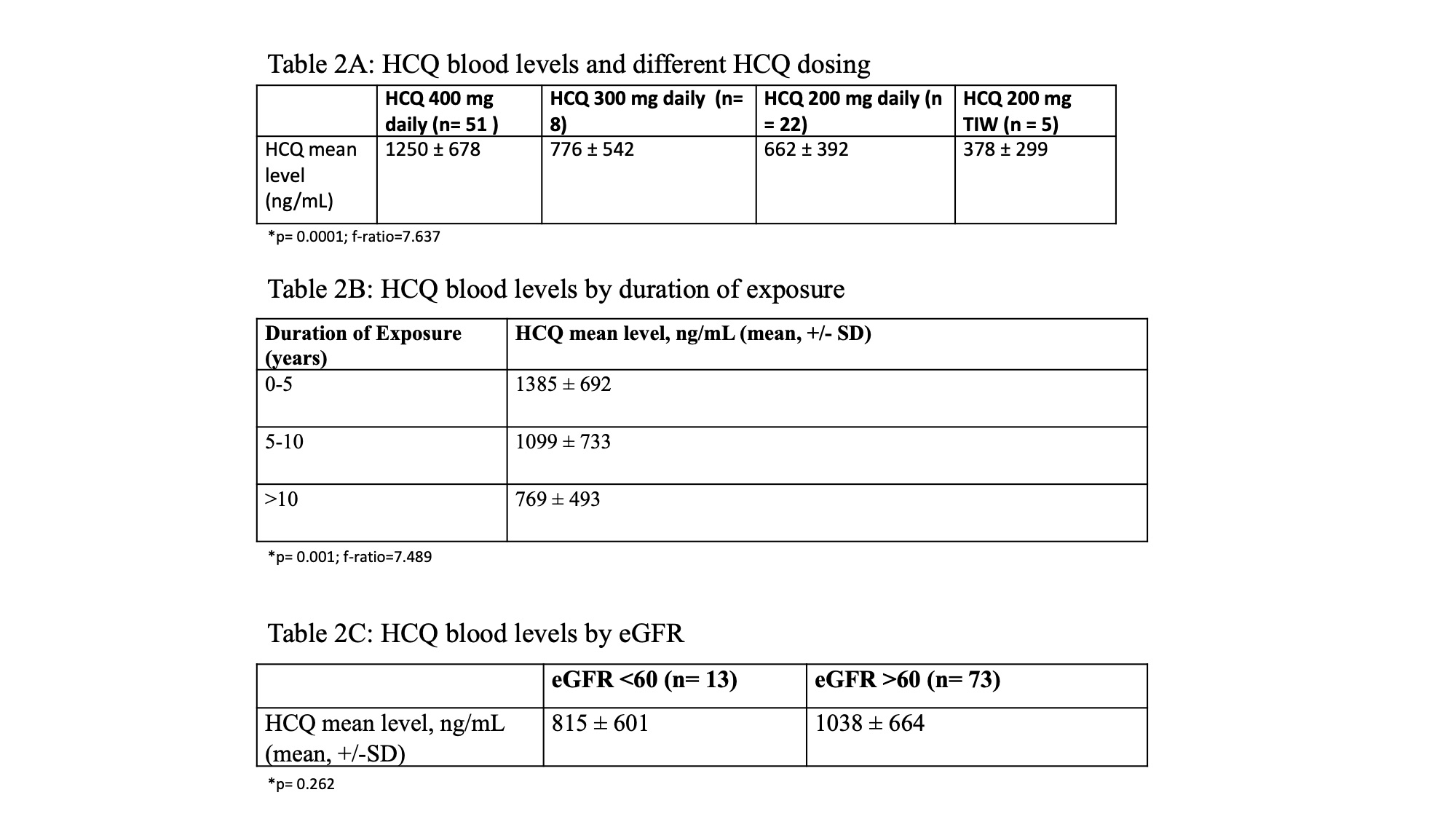
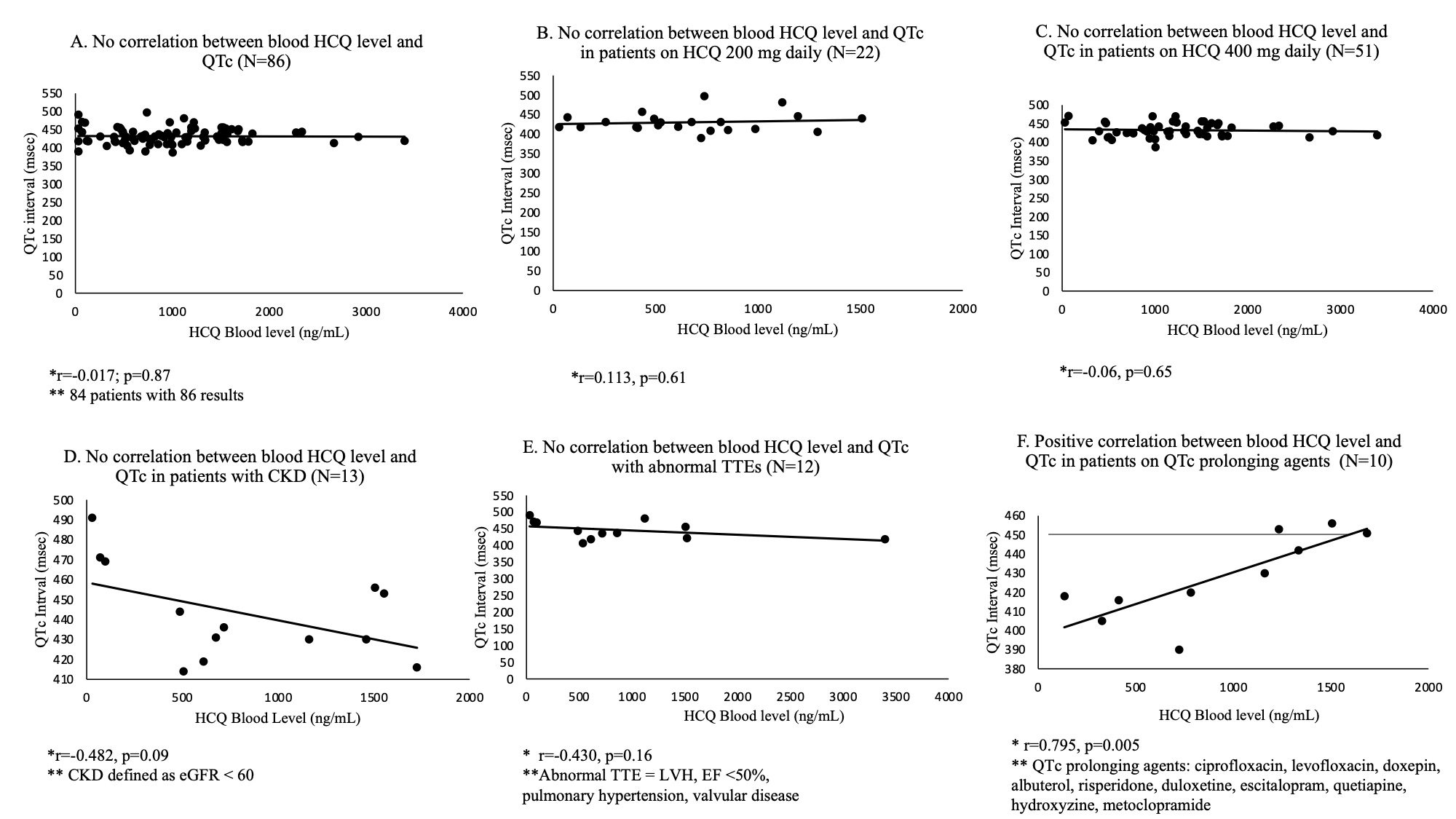
Results: 84 patients, 93% female, 47% European, 35% African, 15% Asian, and 25% Hispanic were included (Table 1). HCQ levels were higher in patients on 400 mg, lower after 10 years of exposure, and unrelated to eGFR (Table 2). There was no correlation between blood HCQ levels and QTc intervals in the 84 patients (r=-0.017; p=0.87) (Fig 1a). Additionally, there was no correlation between blood HCQ levels and QTc intervals in patients on 200 mg or 400 mg of HCQ (r=0.113, p=0.61; r=-0.06, p=0.65) (Fig 1b-c). There was no correlation between blood HCQ levels and QTc intervals in patients who had chronic kidney disease (defined as eGFR < 60), (r=-0.482, p=0.09) or those with underlying cardiac abnormalities noted on transthoracic echocardiogram (r=-0.430, p=0.16) (Fig 1d-e). However, there was a positive correlation between blood HCQ levels and QTc intervals in patients who were on concomitant QTc prolonging agents, (r=0.795, p=0.005). but none in excess of 456 msec (Fig 1f).
Conclusion: Our study provides reassurance that hydroxychloroquine is not associated with QTc prolongation in patients with SLE and across different subsets of patients irrespective of blood level, dose prescribed, CKD or underlying cardiac abnormalities. There was a positive correlation between blood HCQ levels and QTc intervals in patients on concomitant QTc prolonging agents, but none were severely prolonged (eg > 500 msec). This is the first study relying on measured blood levels demonstrating the absence of consequential increase in QTc levels in HCQ treated SLE patients.

To cite this abstract in AMA style:
Haj-Ali M, Belmont H. Whole Blood Hydroxychloroquine Levels Do Not Correlate with QTc Intervals in a Cohort of 84 SLE Patients: Evidence That Antimalarials Are Not Associated with Cardiac Conduction System Toxicity [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/whole-blood-hydroxychloroquine-levels-do-not-correlate-with-qtc-intervals-in-a-cohort-of-84-sle-patients-evidence-that-antimalarials-are-not-associated-with-cardiac-conduction-system-toxicity/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/whole-blood-hydroxychloroquine-levels-do-not-correlate-with-qtc-intervals-in-a-cohort-of-84-sle-patients-evidence-that-antimalarials-are-not-associated-with-cardiac-conduction-system-toxicity/