Session Information
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Vitamin D has effects on the cardiovascular system, including decreased renin-angiotensin, decreased insulin resistance, increased vascular relaxation and decreased vascular smooth muscle cell proliferation, that suggest it should have benefits for cardiovascular risk factors. It already has a role in the control of SLE disease activity, as it in particular reduces the urine protein/cr ratio. We explored this in a longitudinal SLE cohort.
Methods: This analysis included 1,503 patients, contributing 21,216 visits with 25(OH) vitamin D levels from May 2009 to March 2019. They were observed from 1 to 48 visits with a median of 12 visits per patient. 134 patients (9%) had 1 visit, 300 (20%) had 2-5 visits, 234 (16%) had 6-10 visits, and 835 (56%) had 11 or more visits in this analysis. 92% of the patients were female, 50% Caucasian, and 41% African American. At the first visit when 25(OH) vitamin D level was measured, mean age was 42.9 (SD=13.6) years. 20% were under the age of 30, 36% were between the age of 30 and 44, 33% between 45 and 59, and 12% were 60 or older. 77% had their first vitamin D level below 40 ng/mL and 26.5% had their first vitamin D level below 20 ng/mL. Longitudinal regression models between 25(OH) vitamin D levels and cholesterol levels, systolic blood pressure and glucose levels were constructed.
Results: We performed “between” person analyses: whether patients with higher levels of 25(OH) vitamin D had lower levels of the cardiovascular risk factors; serum cholesterol (Table 1), systolic blood pressure (Table 2) and glucose (Table 3). The reduction in serum cholesterol and systolic blood pressure was best fit by a two slope model, with the break point at 50 ng/mL and 40 ng/mL of 25(OH) vitamin D, respectively. Below the break point, the reduction was markedly greater. In a separate analysis, we demonstrated similar benefits in patients over time (“within patient”), with reduced cardiovascular risk factors at visits in which 25(OH) vitamin D levels were higher.
Conclusion: Higher 25(OH) vitamin D levels resulted in significantly lower total cholesterol, lower systolic blood pressure and lower glucose. No additional benefit was achieved above 50 ng/mL (for cholesterol) or 40 ng/mL (for systolic blood pressure). A similar break point of 40 ng/mL was found for the benefit of vitamin D supplementation on SLE disease activity. This “breakpoint” means that the target 25(OH) vitamin D is at a safe level, without risk of toxicity. Given the role of vitamin D in vascular repair and endothelial function, and its anti-inflammatory activity in blocking NF-kappa beta and reducing production of pro-inflammatory cytokines, replacement of vitamin D in SLE patients who are deficient or insufficient should be recommended, both for disease activity and also for long-term cardiovascular benefit.
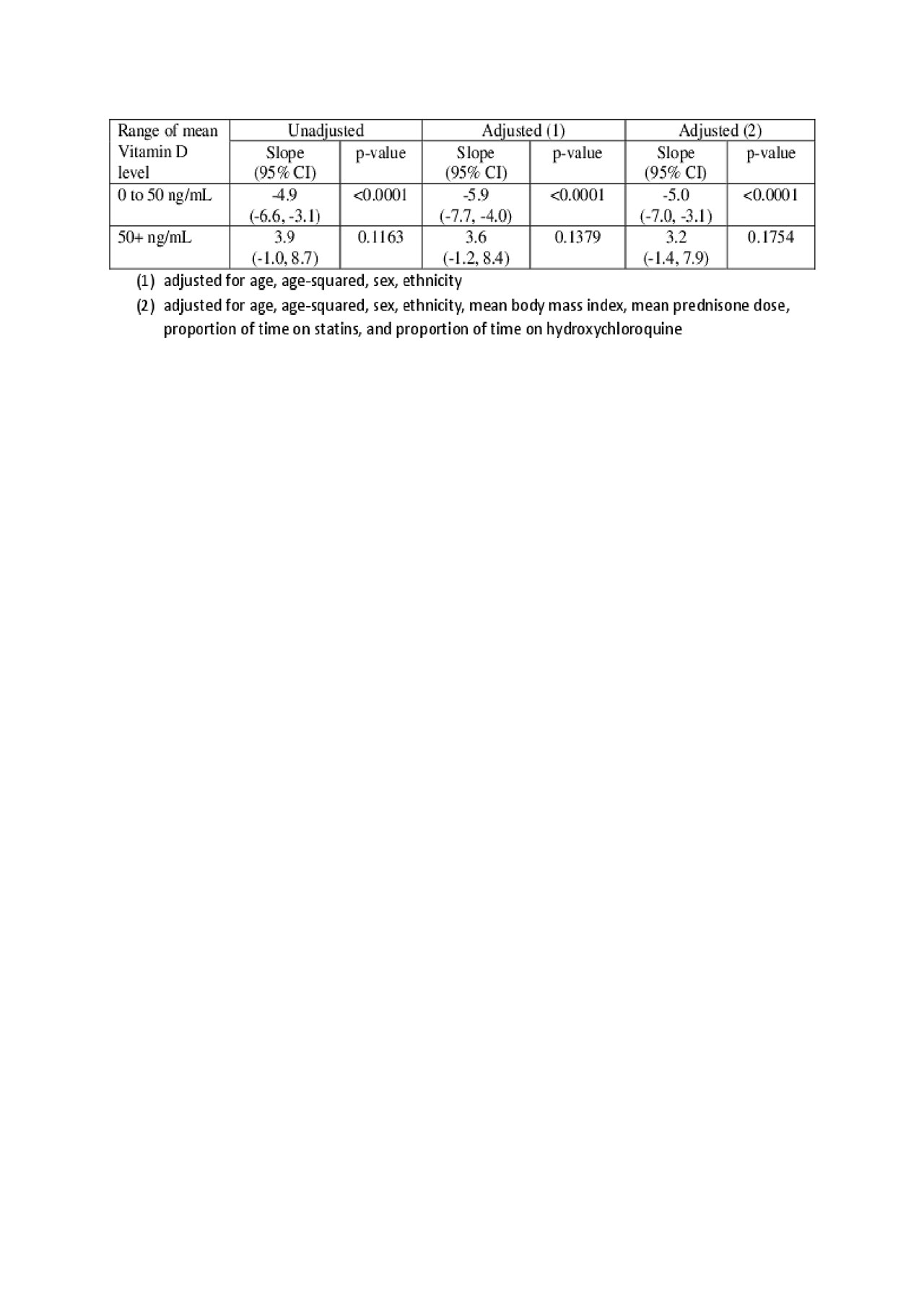
ACR 2019-Vitamin D Lowers CV risk facotrs SLE-Table1
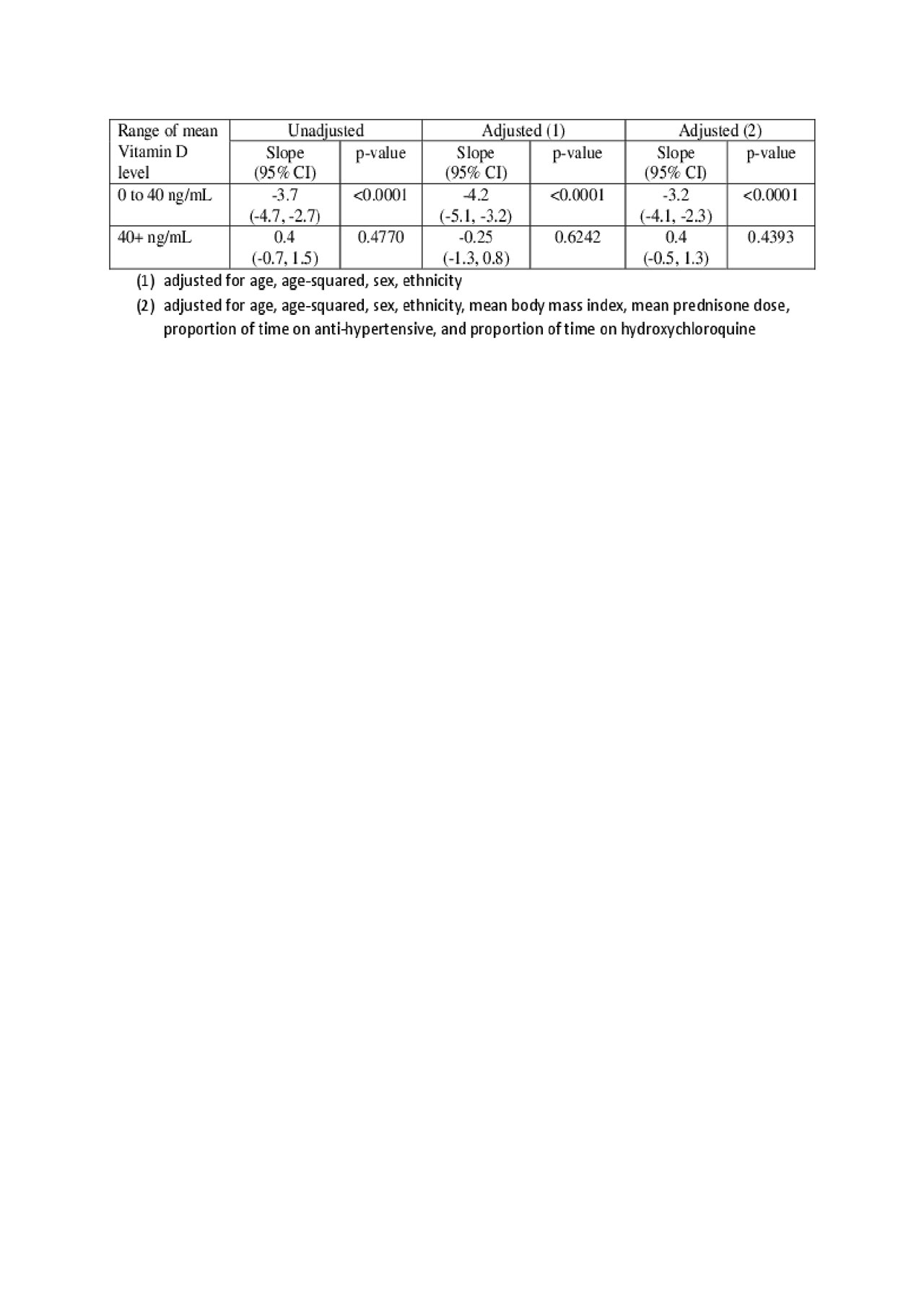
ACR 2019-Vitamin D Lowers CV risk facotrs SLE-Table2
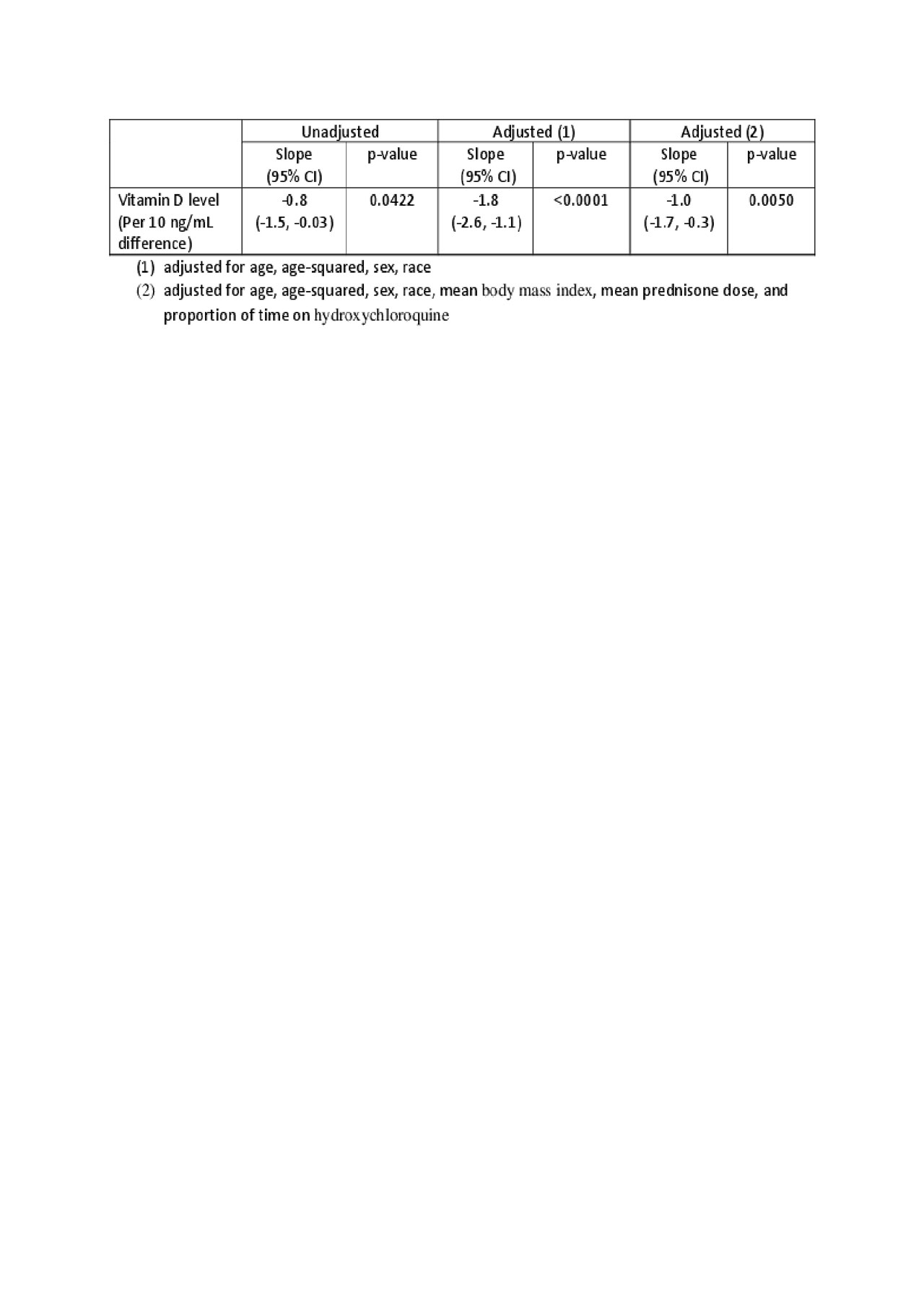
ACR 2019-Vitamin D Lowers CV risk facotrs SLE-Table3
To cite this abstract in AMA style:
Petri M, Li J, Goldman D. Vitamin D Reduces Cardiovascular Risk Factors in SLE [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/vitamin-d-reduces-cardiovascular-risk-factors-in-sle/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/vitamin-d-reduces-cardiovascular-risk-factors-in-sle/