Session Information
Date: Sunday, November 5, 2017
Title: Rheumatoid Arthritis – Clinical Aspects I: Cardiac Comorbidities
Session Type: ACR Concurrent Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Rheumatoid arthritis (RA) patients have a greater risk of cardiovascular (CV) mortality compared to general population. Traditional CV risk factors may be less accurate in predicting CV mortality in RA patients. We examined the performance of the CV risk factors compared to carotid ultrasound measures of intima-media thickness (IMT) in predicting CV mortality in a RA cohort.
Methods: We recruited patients who met the 1987 ACR criteria for RA from private, public and military rheumatology practices. We measured carotid IMT using high resolution ultrasound. Baseline data on traditional CV risk factors which included systolic blood pressure, diabetes, smoking, high density lipoprotein and total cholesterol were collected. For Framingham CV risk, we used published tables to calculate the predicted 10-year risk of coronary heart disease, based on the above risk factors. We then divided Framingham risk score into three categories defined as low (<10%), intermediate (10-20%) and high (>20%) risk of CV mortality. We also divided IMT into risk groups of low (IMT < 1.0 mm), intermediate (IMT 1.0-1.5 mm) and high (IMT > 1.5 mm). Patients were followed prospectively until they either died or reached the censoring date of Nov 12, 2015. Certificates were obtained for all deaths, and cause of death classified as CV according to established criteria. We then plotted area receiver operator characteristic (ROC) curves, calculated the area under the curve (AUC) and compared curves using Stata 8.2. We also computed the Net Reclassification Index (NRI).
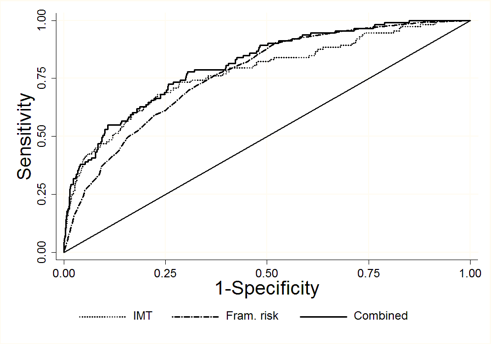
Results: We followed 1,194 RA patients for 7,062 patient years. During this time, 113 CV related deaths occurred, for a CV mortality rate of 1.6 per 100 patient-years. Both the Framingham risk score and the carotid IMT were significantly associated with CV mortality. Patients in the high Framingham risk group had a CV mortality rate of 5.7 per 100 patient years, while those in the lower risk group had a CV mortality rate of 0.8 per 100 patient years. Patients in high IMT category had a CV mortality rate of 5.8 per 100 patient years, while those in the low IMT category had a CV mortality rate of 0.6 per 100 patient years. The ROC area for the Framingham risk score was 0.7695 and while that of carotid IMT was 0.7760 (P=ns). When combined the Framingham risk score with the carotid IMT, the ROC curve area increased to 0.8096 (P < 0.0001, Figure). The carotid IMT added to the Framingham risk score, correctly reclassified 12.6% of the patients (NRI of 0.126, p=0.01).
Conclusion: Our findings suggest that carotid ultrasound measures of IMT significantly increase accuracy of CV mortality predictions in RA patients over Framingham risk score.
To cite this abstract in AMA style:
Gupta P, Escalante A, Battafarano DF, Restrepo JF, del Rincon I. Utility of Carotid Ultrasound Compared to Framingham Risk Score in Predicting Cardiovascular Mortality in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/utility-of-carotid-ultrasound-compared-to-framingham-risk-score-in-predicting-cardiovascular-mortality-in-rheumatoid-arthritis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/utility-of-carotid-ultrasound-compared-to-framingham-risk-score-in-predicting-cardiovascular-mortality-in-rheumatoid-arthritis/