Session Information
Date: Tuesday, November 15, 2016
Title: Muscle Biology, Myositis and Myopathies - Poster II: Clinical
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Inclusion body myositis (IBM) is the most common idiopathic inflammatory myopathy in patients over the age of 50. For atypical or early cases where classic histopathologic changes are lacking, imaging can play a role in identifying subclinical muscle involvement. Muscle sonography has shown an increased muscle echointensity (EI) seen in various disease states. This study was undertaken to assess the pattern of muscle involvement in IBM patients with the use of ultrasound and identify potential imaging features of the disease.
Methods: Patients seen from November 2015 to May 2016 with clinicopathologically or clinically defined IBM by European Neuromuscular center were included in the study. Seven muscle groups were imaged bilaterally for each patient (deltoids, biceps, flexor carpi ulnaris, flexor digitorum profundus, rectus femoris, tibialis anterior and gastrocnemius) using a standardized protocol. Images were coded for muscle severity qualitatively using the Heckmatt score (1 normal, 2 slightly increased muscle EI, 3 marked increase in EI with decreased bone echo, and 4 severely increased EI with no bone echo). Quantitative values for muscle echointensity were calculated for each muscle by manually segmenting each muscle through ITK-Snap and calculating average pixel intensity through MATLAB. Mean values were calculated for each muscle group.
Results: Sixteen patients were included in the study, 8 male and 8 female, all Caucasian. Average duration of disease was 11.8 years. Of the 7 muscle groups studied, the muscles showing the most severe abnormalities with a Heckmatt score of 3 or more were the gastrocnemius and flexor digitorum profundus. Quantitative assessment of echointensities similarly showed the highest values for the gastrocnemius, flexor digitorum profundus and the biceps. There was also asymmetry often seen between muscle groups of the same patient, particularly in the gastrocnemius, with a heterogeneously increased EI, often in a “popcorn pattern”.
Conclusion: Muscle sonography can be a useful adjunct evaluation in patients suspected to have inclusions body myositis. Findings are a heterogenously increased echogenicity in affected muscles. Most severely affected muscle groups tended to be the gastrocnemius and flexor digitorum profundus. The presence of asymmetry between sides may also be an additional indicator of the disease.
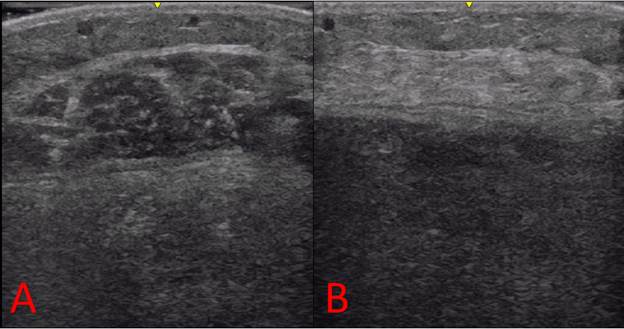
Figure 1. Asymmetry of appearance of gastrocnemius in same patient: A left, B right
 Figure 2. Heterogenous increase in EI of gastrocnemius muscle (“popcorn pattern”)
Figure 2. Heterogenous increase in EI of gastrocnemius muscle (“popcorn pattern”)
| Muscle | Heckmatt score, mean | Echointensity, mean |
| Deltoids | 2.58 | 80.2 |
| Biceps | 2.84 | 90.72 |
| Flexor carpi ulnaris | 2.84 | 78.54 |
| Flexor Digitorum Profundus | 3.37 | 90.73 |
| Rectus femoris | 2.93 | 80.35 |
| Tibialis anterior | 2.9 | 89.2 |
| Gastrocnemius | 3.37 | 91.28 |
Table 1. Averaged echointensities per muscle group by quantitative and qualitative assessments
To cite this abstract in AMA style:
Albayda J, Paik JJ, Bingham C III, Christopher-Stine L, Chung T, Burlina P, Billings S. Ultrasound Imaging in Inclusion Body Myositis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/ultrasound-imaging-in-inclusion-body-myositis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/ultrasound-imaging-in-inclusion-body-myositis/