Session Information
Session Type: ACR Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Inflammation and new bone formation in the axial skeleton are characteristic features of radiographic axial spondyloarthritis (r-axSpA). Facet joints are frequently involved in r-axSpA but rather difficult to visualize on conventional radiography (CR). However, we have recently shown that low-dose CT (ldCT) can be used to assess facet joint ankylosis in the whole spine, except for the cervicothoracic junction, in patients with r-axSpA. We now aimed to study progression of facet joint ankylosis over two years in patients with r-axSpA.
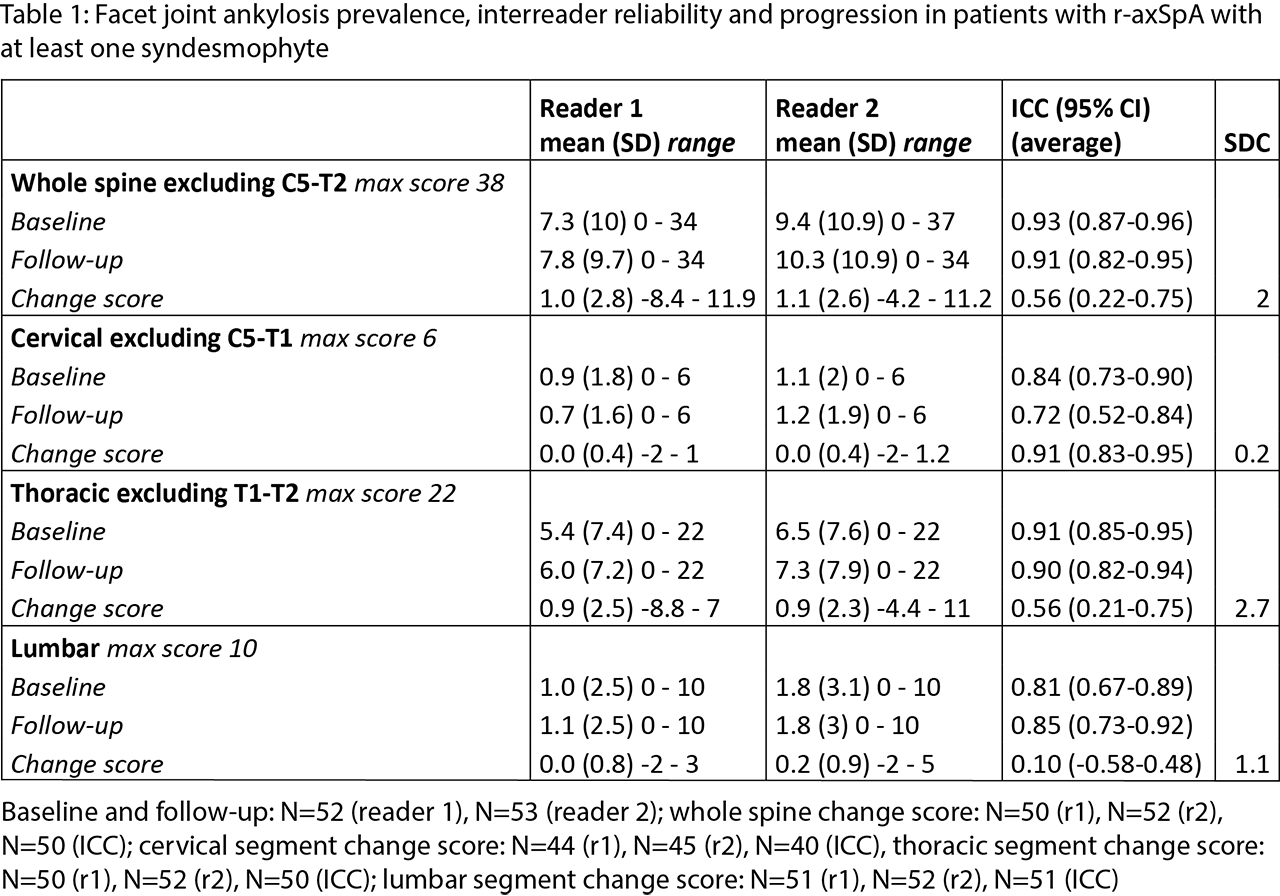
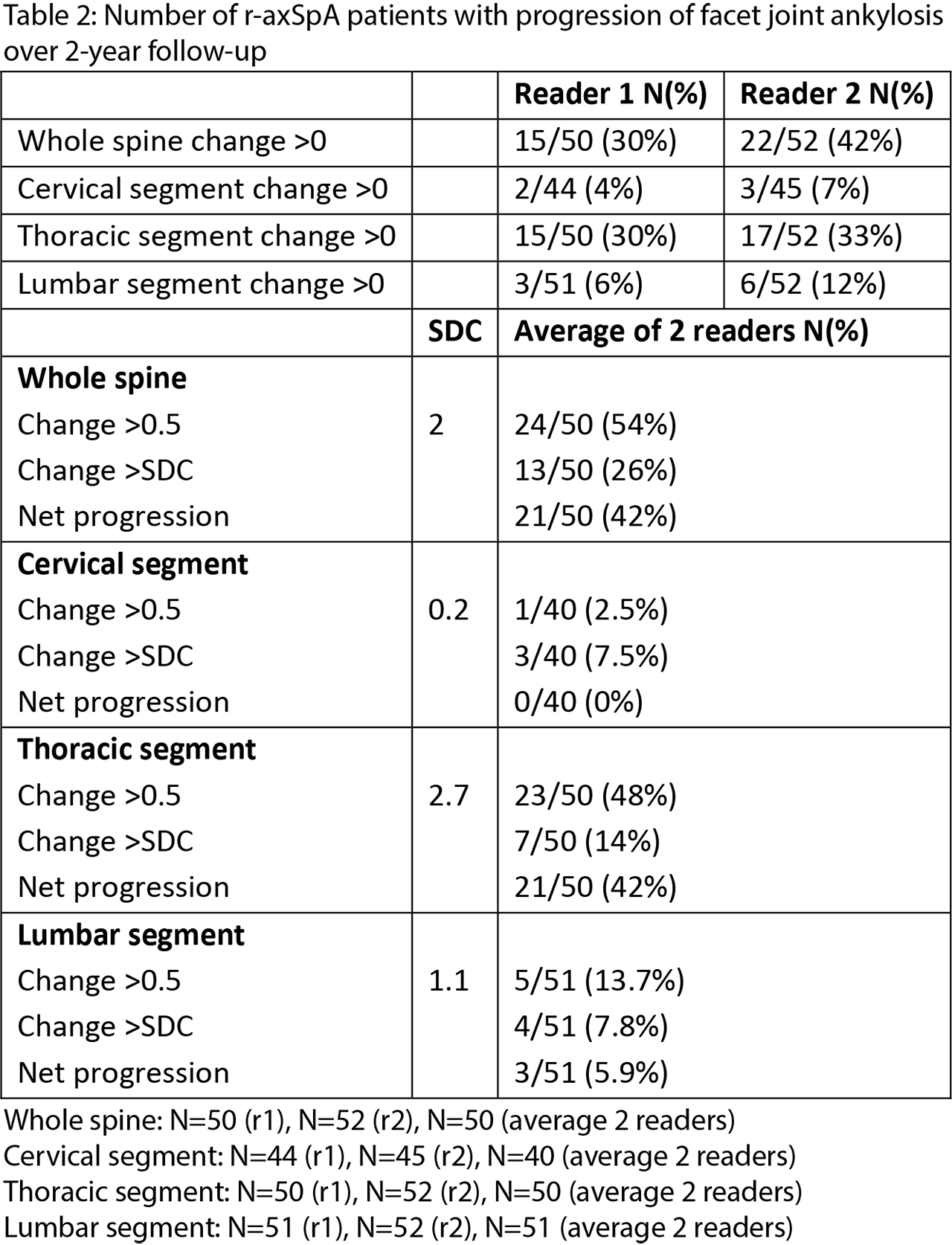
Methods: In an observational cohort, r-axSpA patients with syndesmophytes on ≥1 but no more than 75% of spinal levels of the cervical and lumbar segments on CR and ≥1 inflammatory lesion on spinal MRI underwent whole spine ldCT (about 4 mSv) with repeated ldCT after 2 years. Paired ldCTs were independently assessed by 2 trained readers, blinded to chronology. Left and right facet joints of all levels between C2 and S1, with the exception of the levels between C5 and T2, were scored as ankylosis present (1) or absent (0). Interreader reliability was assessed with intraclass correlation coefficients (ICCs) (two-way average, absolute agreement) and smallest detectable change (SDC). Status scores were calculated for baseline and follow-up. Change scores of the whole spine and per segment were calculated if < 25% of the joint scores were missing. Remaining missing scores were imputed with the mean segment change score. For each reader, progression was calculated as the proportion of patients with change score >0. For the average score of the readers, progression was given as change score >0.5 and >SDC as well as net progression, defined as the number of patients with change score >0.5 minus the number of patients with change score < -0.5 divided by the total number of patients.
Results: Baseline and 2-year follow up ldCT were available in 53 patients with r-axSpA (mean age 48.3, 85% male, 79% HLA-B27+). Interreader reliability for status scores was good to excellent. For change scores this was poor to excellent (table 1). SDCs were relatively low (tables 1 and 2). The proportion of patients with progression is given in table 2. Most changes were seen in the thoracic spine (tables 1 and 2).
Conclusion: Over two years, a fair number of patients had progression of facet joint ankylosis with most progression occurring in the thoracic spine. These results show that using whole spine ldCT, progression of facet joint ankylosis can provide useful information on new bone formation in r-axSpA patients.
To cite this abstract in AMA style:
Stal R, van Gaalen F, Sepriano A, Braun J, Reijnierse M, van der Heijde D, Baraliakos X. Two-Year Progression of Facet Joint Ankylosis on Whole Spine Low-Dose CT in Patients with Radiographic Axial Spondyloarthritis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/two-year-progression-of-facet-joint-ankylosis-on-whole-spine-low-dose-ct-in-patients-with-radiographic-axial-spondyloarthritis/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/two-year-progression-of-facet-joint-ankylosis-on-whole-spine-low-dose-ct-in-patients-with-radiographic-axial-spondyloarthritis/