Session Information
Session Type: Abstract Submissions (ACR)
The high risk of ischemic heart disease (IHD) in patients with rheumatoid arthritis (RA) has been linked to inflammation and disease severity. Treatment with tumour necrosis factor inhibitors (TNFi) can modify cardiovascular risk factors and are often effective in reducing disease activity. The objective of the study was to evaluate the risk of acute coronary syndromes (ACS) in patients treated with TNFi for RA compared with the risk in bio-naïve RA patients and in the general population.
Methods:
In the Swedish Biologics Register we identified a cohort of patients, with RA and no previous IHD, starting their first TNFi 2001-2010 (n=7,704, mean age 57.1 years, 75.9% women). Matched bio-naïve referents were randomly selected (3:1, n=23,112) from the underlying national cohort of all individuals with two or more outpatient diagnoses of RA (one of which at a dept. for Rheumatology or internal medicine) as identified in the National Patient Register. Furthermore, a matched comparator cohort (5:1, n=38,520) was randomly selected from the Population Register. Covariates were obtained from the Patient register (joint surgery, disease duration, and prevalent diagnoses of hypertension, diabetes, chronic pulmonary disease, infection, cerebrovascular disease and other atherosclerotic disease,) and Statistics Sweden (educational level and previous work disability). Three exposure windows were defined; Actively on TNFi – Until date of termination of TNFi therapy +90 days, Short term exposure – limiting the follow-up on TNFi to 2 years, and Ever exposed to TNFi. The outcome, incident ACS, was defined as a primary discharge diagnosis of myocardial infarction, or unstable angina, or myocardial infarction as the underlying cause of death. Incidence rates were calculated and Cox Proportional Regression models were utilized for risk estimations.
Results:
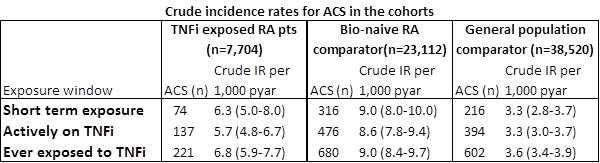
The fully adjusted hazard ratios, HR (95%CI), for TNFi exposed compared with bio-naïve RA patients were for Short term exposure 0.78 (0.61-1.01), Actively on TNFi 0.73 (0.60-0.89), and Ever exposed 0.82 (0.70-0.95). Comparing the bio-naïve RA cohort with the general population fully adjusted models resulted in the HRs Short term exposure 2.27 (1.88-2.73), Actively on TNFi 2.10 (1.82-2.43), and Ever exposed 2.03 (1.80-2.29) for the risk of ACS. The corresponding HRs for the TNFi cohort compared with the general population referents were 1.65 (1.23-2.22), 1.50 (1.21-1.85), and 1.61 (1.36-1.92) respectively.
Conclusion:
In this nation-wide, population-based, matched cohort study treatment with TNFi was associated with a modest reduction of the risk of ACS in patients with RA. Compared with the general population the risk of ACS in RA was increased, although less pronounced among the TNFi exposed patients. The decrease in risk could be attributable to the TNFi per se, or correspond to a higher degree of inflammatory control in the treatment group.
Disclosure:
L. Ljung,
Bristol Myers Squibb,
5;
J. Askling,
Pfizer Inc,
2;
S. M. Rantapää-Dahlqvist,
None;
L. T. H. Jacobsson,
Pfizer ,
2,
Pfizer ,
5,
UCB,
5,
Abbvie ,
5;
T. ARTIS Study Group,
Merck, BMS, Pfizer, Abbott Laboratories, SOBI, UCB, and Roche,
9.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/tumour-necrosis-factor-inhibitors-and-the-risk-of-acute-coronary-syndrome-in-rheumatoid-arthritis-a-national-cohort-study/