Session Information
Date: Tuesday, November 7, 2017
Title: Systemic Sclerosis, Fibrosing Syndromes and Raynaud's – Clinical Aspects and Therapeutics Poster III
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Title: Troponinemia independently associates with mortality in systemic sclerosis
Background/Purpose: Cardiac involvement is common in systemic sclerosis (SSc) and in the early asymptomatic stages, elevated troponin, or troponinemia, may be the only sign of ongoing myocardial disease.
Methods: This retrospective, cross-sectional study included SSc patients with any troponin measurement in the past 10 years, as identified using our institution¡¯s electronic medical record system. Elevated troponin was defined as any value above or at the cut off of normal value in a commercially available laboratory. Clinical data including SSc subtype, disease duration, maximum modified Rodnan skin score (mRSS), maximum serum creatine kinase, aldolase, pro-B-type natriuretic peptide (BNP), echocardiographic and right heart catheterization data were compared between those with elevated troponin and normal troponin. Survival analyses including Cox proportional hazards regression analyses were used to compare both groups.
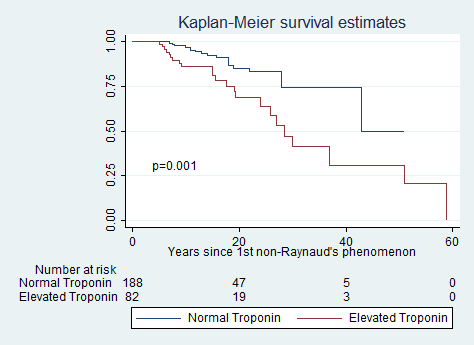
Results: 272 patients were identified with a troponin evaluated during the study period. 83 (31%) had an elevated troponin. Compared to those with a normal troponin, SSc patients with troponinemia were more likely to have the diffuse SSc subtype (55% vs. 37%, p=0.004), shorter disease duration since first non-Raynaud¡¯s symptom (5.8 ± 8.4 vs. 6.1 ± 7.6 years; p=0.30), lower ejection fraction (EF) (49.8 ± 12 vs. 54.8 ± 7.3, p=<0.0001), lower FVC (61.2 ± 18.8 vs. 66.8 ± 20.4, p=0.03), higher RVSP( 51.7 ± 21.2 vs. 43.8 ± 16.2, p=0.002), more renal crisis (8.4% vs. 2.6%, p=0.04), higher Medsger muscle (p=0.001) and heart severity scores (p=0.001). Patients with troponinemia also have higher CK values (514 ± 783 vs. 300 ± 553, p=0.01) and higher aldolase (15 ± 11 vs. 11.3 ± 6.3, p=0.002). There was higher frequency of death (28% vs. 9.5%, p=<0.0001). Cox proportional regression analyses demonstrated that patients with troponinemia are 3.2 times (95% confidence interval, 1.33 to 7.7, p=0.009) more likely to have death than those without an elevated troponin even after controlling for SSc subtype, age, gender, race, duration of disease, diabetes, coronary artery disease, smoking, CK, BNP, and World Health Organization dyspnea classification.
Conclusion: SSc patients with troponinemia have increased all-cause mortality when compared to those without an elevated troponin even after controlling for demographic and disease-specific confounders.
|
Clinical Characteristics |
Troponin Positive (N=83) |
Troponin negative (N=189) |
p-value |
|
Disease duration defined by 1st non-Raynaud¡¯s (at first visit) |
5.8 ± 8.4 years |
6.1 ± 7.6 years |
0.79 |
|
Age at SSc diagnosis defined by 1st non-Raynaud¡¯s |
45.7 ± 14.2 years |
44 ± 13.9 years |
0.34 |
|
Female |
60 (72.3%) |
154 (81.5%) |
0.06 |
|
Diffuse skin subtype |
46 (55.4%) |
70 (37%) |
0.004 |
|
Renal crisis |
7 (8.4%) |
5 (2.6%) |
0.04 |
|
Race Caucasian African-American Other |
46 (55.4%) 34 (41%) 3 (3.6%) |
122 (64.6%) 59 (31%) 8 (4.2%) |
0.30 |
|
Maximum Heart Severity Score 0 1 2 3 4 |
25 (30.9%) 4 (4.9%) 10 (12.4%) 2 (2.5%) 40 (49.4%) |
102 (55.1%) 11 (6.0%) 22 (11.9%) 5 (2.7%) 45 (24.3%) |
0.001 |
|
Maximum Muscle Severity Score 0 1 2 3 4 |
32 (38.6%) 37 (44.6%) 10 (12.1%) 2 (2.4%) 2 (2.4%) |
123 (65.1%) 48 (25.4%) 12 (6.4%) 2 (1.1%) 4 (2.1%) |
0.001 |
|
Maximum RVSP |
51.7 ± 21.2 |
43.8 ±16.2 |
0.002 |
|
Max pro-BNP |
6205 ± 22110 |
896 ± 1833 |
0.003 |
|
Lowest Ejection Fraction |
49.8 ± 12 |
54.8 ± 7.3 |
<0.0001 |
|
Lowest FVC |
61.2 ± 18.8 |
66.8 ± 20.4 |
0.03 |
|
Coronary Artery Disease |
16 (19.5%) |
21 (11.2%) |
0.06 |
|
Ever Smoker |
34 (41%) |
74 (39.2%) |
0.44 |
|
Dyslipidemia |
30 (37%) |
68(37%) |
0.53 |
|
Diabetes |
9 (10.8%) |
8(4.3%) |
0.04 |
|
Peripheral artery disease |
10 (12.2%) |
12 (6.5%) |
0.09 |
|
History of myopathy |
48 (52%) |
57(30.2%) |
0.001 |
|
Maximum CK |
514 ± 783 |
300 ± 553 |
0.01 |
|
Maximum aldolase |
15.0 ± 11 |
11.3 ± 6.3 |
0.002 |
|
Deceased |
23 (27.7%) |
18 (9.5%) |
<0.0001 |
|
Anti-centromere |
12 (23.5%) |
32 (23.9%) |
0.56 |
|
Anti-topoisomerase 1 |
13 (26.5%) |
27 (21.3%) |
0.29 |
|
Anti-U1RNP |
4 (10.8%) |
9 (8.9%) |
0.50 |
|
Anti-RNA Poly III |
7 (21.2%) |
10 (13.2%) |
0.22 |
To cite this abstract in AMA style:
Paik JJ, Choi D, Wigley FM, Hummers LK, Shah AA. Troponinemia Independently Associates with Mortality in Systemic Sclerosis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/troponinemia-independently-associates-with-mortality-in-systemic-sclerosis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/troponinemia-independently-associates-with-mortality-in-systemic-sclerosis/