Session Information
Date: Sunday, November 8, 2020
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Pharmacological management of cardiac sarcoidosis (CS) includes immunosuppressive therapy for active lesions, guideline-directed medical therapy for heart failure, and antiarrhythmics. Our goal was to observe the various clinical characteristics of CS patients, choice of treatment plans, and outcomes of therapy via analysis of standardized uptake values (SUV) and ejection fraction (EF) using pre- and post-treatment cardiac PET-CT.
Methods: The data was gathered by retrospective chart review of 31 patients treated at our institute with a diagnosis of CS (as defined by the Heart Rhythm Society diagnostic criteria). Patients having at least two PET scans spaced at least 6 months apart were included, and they had to be on a stable treatment regimen for at least 6 months prior to their follow up PET-CT. Changes in medications were noted.
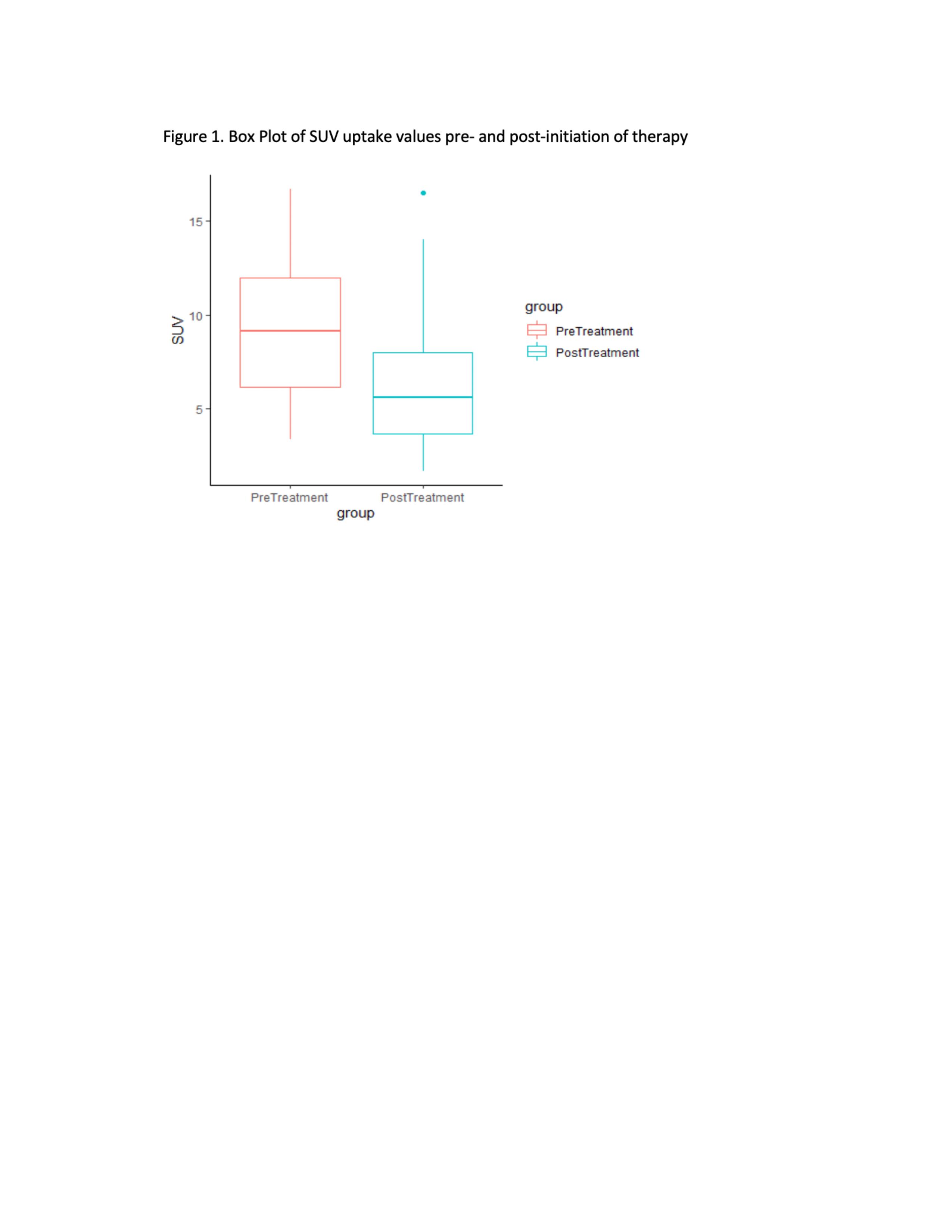
Results: Table 1 summarizes patient’s baseline clinical characteristics, diagnostic workup, treatments and the changes in SUV and EF using pre- and post-treatment PET-CT. The average time between first PET-CT and therapy initiation was 4.3 months and the average time between therapy initiation and follow-up PET-CT was 14.5 months. The average SUV uptake before starting any therapy was 9.2 ± 3.64, which decreased to 5.98 ± 3.67 on follow-up assessment (Figure 1). The average difference between pre- and post-treatment SUV was -3.22 (SD=5.39, 95% CI: -5.23, -1.21) with paired t-test (p-value=0.002) suggesting improvement in mean SUV with therapy. The average difference between pre- and post-treatment ejection fraction was 0.13% (95%CI: -3.5%, 3.8%) with paired t-test (p=0.94) suggesting no difference.
MTX was used most commonly as initial therapy followed by AZA, HCQ, LEF and MMF. Many treatment combinations also used background therapy with prednisone. The most common biologic used was infliximab followed by adalimumab. A sunburst plot provides a representation of the sequence of medications use in this cohort of CS patients (Figure 2). Patients were divided into a MTX treatment group (n=16) where MTX formed the backbone of therapy with or without HCQ (n=2) or prednisone (n=10). A second group termed the ‘Other treatment group’ (OT group) was formed for analysis consisting of: AZA monotherapy (n=1), AZA in combination with prednisone (n=1), prednisone monotherapy (n=1) and MMF in combination with prednisone (n=2). The baseline SUV max was similar in the MTX and OT groups (9.2 vs 10.4) as was the EF (52% vs 46%). There was a difference in the interval between the baseline cardiac PET-CT and the initiation of medical therapy in the MTX group vs the OT group (4 months vs 0.5 months). The change in SUV max was slightly greater in the OT group when compared to the MTX group (-5.6 vs -3.5), though the change in EF was similar (-3% vs 2%).
Conclusion: We described the clinical characteristics and treatment patterns of 31 patients with CS. We did not observe a pronounced difference between the MTX and the OT group with respect to SUV patterns and EF before and after initiating therapy. Further large-scale prospective studies are required to identify the most effective treatment regimen in the management of CS.


To cite this abstract in AMA style:
Gill R, Lavellee M, Petrides M, Ford S, Kowlgi G, Syed H, Sima A. Trend of Treatment Plans, and Outcomes of Therapy in Cardiac Sarcoidosis via Analysis of Standardized Uptake Values Score and Ejection Fraction Using a Cardiac PET-CT [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/trend-of-treatment-plans-and-outcomes-of-therapy-in-cardiac-sarcoidosis-via-analysis-of-standardized-uptake-values-score-and-ejection-fraction-using-a-cardiac-pet-ct/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/trend-of-treatment-plans-and-outcomes-of-therapy-in-cardiac-sarcoidosis-via-analysis-of-standardized-uptake-values-score-and-ejection-fraction-using-a-cardiac-pet-ct/