Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: To compare physicians’ opinion on
and adherence to treatment study protocols targeted at either Disease Activity
Score (DAS) ≤2.4 or <1.6.
Methods: The BeSt
study compared
4 treatment strategies in 508 early rheumatoid arthritis (RA, 1987
criteria)
patients,
targeted
at DAS ≤2.4, at 3 monthly evaluations. Seven years later, in roughly the
same rheumatology clinics, the IMPROVED study started with methotrexate and
prednisone in 479 early RA (2010 criteria) and 122 undifferentiated arthritis
(UA) patients, followed by 2 randomization arms targeted at DAS remission (<1.6),
at 4 monthly evaluations. We evaluated physicians’ adherence to the
protocols and assessed associated opinions and conditions during 4 year follow
up by Generalized Linear Mixed Models (GLMM).
Results: Protocol
adherence (PA) over 4 years was higher in BeSt than in IMPROVED (mean over time
88% and 69%, respectively). PA decreased during follow up in both studies from
100% to 77% (BeSt) and to 55% (IMPROVED). Protocol violations (PV) occurred in
IMPROVED in (mean over time) 23% and in BeSt in 12%. In IMPROVED, more PV were
against required treatment intensification/restart (64%), compared to 33% against
required drug tapering/discontinuation, whereas in BeSt this was almost similar
(47% and 42%, respectively). Where the physician incorrectly didn’t taper/stop,
the measured DAS was (median 0.6 (IQR -0.9;-0.3)) lower than the target DAS
<1.6 (IMPROVED) and (0.7 (-1.2;-0.3)) lower than target DAS≤2.4 (BeSt).
Where they incorrectly didn’t intensify/restart, the measured DAS was (0.5 (0.2;0.8))
above the DAS target <1.6 (IMPROVED), and (0.7 (0.3;1.3)) above target DAS≤2.4
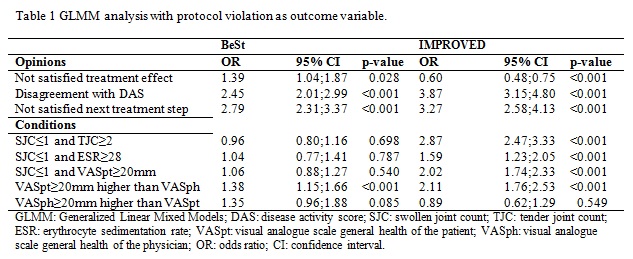
(BeSt). In BeSt the odds for PV were higher if physicians were not satisfied
with the current treatment effect, disagreed with the DAS, or with the next
treatment step (table 1). In IMPROVED the odds for PV were higher if physicians
disagreed with the DAS or with the next treatment step, but disagreement with
the current treatment effect was associated with fewer PV. We formulated
conditions where objective and subjective measures of disease activity
differed, and might therefore induce a higher risk for PV. In table 1 the odds
for PV associated with these conditions in the BeSt and IMPROVED are shown.
Conclusion: Physicians
mostly followed both DAS steered treatment study protocols but over 4 years
follow up PA decreased in both studies and more in the IMPROVED. Where the
protocol was not followed, the difference between measured and target DAS
appeared smaller in the IMPROVED than in the BeSt. A DAS slightly over target (>1.6)
requiring drug intensification resulted in more PV than a DAS under the target
requiring drug tapering in the IMPROVED. These results may indicate that physicians
intend to follow a DAS <1.6 steered protocol but especially reluctant to
increase therapy when elements of a DAS >1.6 may not represent true disease
activity.
To cite this abstract in AMA style:
Akdemir G, Markusse IM, van Groenendael JHLM, Peeters AJ, Molenaar ET, Kerstens PJSM, Lems WF, Huizinga TWJ, Allaart CF. Treatment Target in a Disease Activity Score Steered Treatment Protocol in Early Arthritis Patients: Low Disease Activity or Remission [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/treatment-target-in-a-disease-activity-score-steered-treatment-protocol-in-early-arthritis-patients-low-disease-activity-or-remission/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/treatment-target-in-a-disease-activity-score-steered-treatment-protocol-in-early-arthritis-patients-low-disease-activity-or-remission/