Session Information
Session Type: ACR Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Treat to Target (T2T) opportunities and rheumatologist decision making are not defined, captured, or reportable within existing electronic health record (EHR) software. We developed a novel EHR-integrated electronic system that 1) signals rheumatologists in real time of an escalation or de-escalation treatment opportunity, 2) captures their decision making including exceptions, and 3) reports on those decisions.
Methods: Using the CDAI (Clinical Disease Activity Index – disease activity measure), we electronically defined an Escalation Opportunity (E-Opp) as the 2 most recent CDAIs in the moderate or high disease activity range and a De-escalation Opportunity (D-Opp) as every CDAI for the past year in the low or remission range.
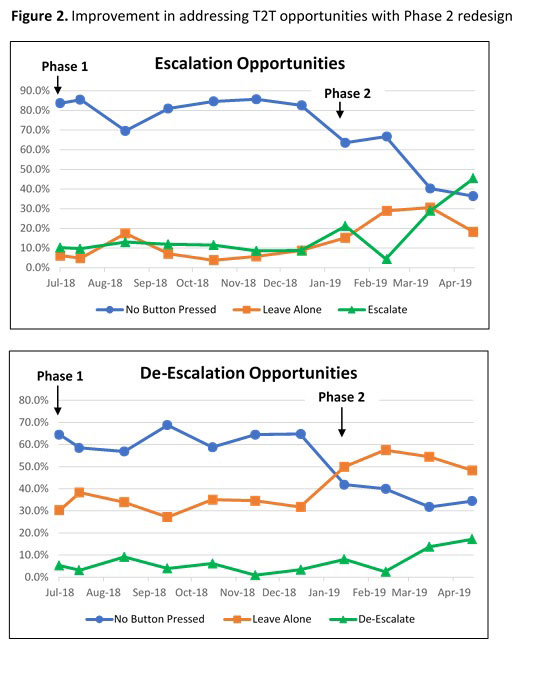
Using EHR-integrated software that captures CDAI measures, we designed a T2T tab that displayed the E-Opp or D-Opp (Phase 1). The rheumatologist could choose to escalate/de-escalate therapy, or leave alone and why. The system then deactivated display of future T2T opportunities for that patient for a defined time period to minimize physician burden. Because of low adoption of navigation to the T2T tab, the software was redesigned (Phase 2) to give a visual cue upon completion of the CDAI, prompting in real time to address the T2T opportunity (Figure 1).
Results: Between July 2018 and early May 2019, there were 1,428 T2T opportunities, representing 34.2% of the completed RA office visits during that time period. 11.3% of RA visits had an E-Opp and 22.9% of RA visits had a D-Opp. During Phase 1, rheumatologists used the T2T tab for only 18.1% of the E-Opp and 37.5% of the D-Opp. At the end of Phase 2, T2T tab use had risen to 63.6% for E-Opp and 65.5% for D-Opp (Figure 2). A decision to escalate rose from 10.2% to 45.5% of all E-Opp, and a decision to de-escalate rose from 5.3% to 17.2% of all D-Opp.
For opportunities where a decision was made, rheumatologists selected “leave alone” for 48.9% of E-Opp and 80.0% of D-Opp. When there was an E-Opp, reasons for “leave alone” included CDAI measure not accurate (33.9%), patient decision (14.5%), risk > benefit (14.5%), other (37.1%). When there was a D-Opp, reasons for “leave alone” included hard to control (46.1%), patient preference (29.4%), and poor prognostic factors (24.5%).
Conclusion: We designed and tested an EHR-integrated Treat to Target (T2T) tool that prompted rheumatologists about escalation/de-escalation opportunities and captured their medical decision making. Opportunities for escalation and de-escalation of therapy are common (34.2 % of RA visits), even in a well-managed RA population. Adoption of T2T tool use improved significantly with real-time visual notification. In parallel, decisions to escalate and de-escalate when opportunities existed also rose (10.2% to 45.5%, and 5.3% to 17.2%, respectively). Using this novel tool, the ability to reliably capture why escalation/de-escalation opportunities are deferred (“leave alone”) will allow us to develop refined T2T care strategies. Now that it is embedded in routine RA care, next steps will be to use this tool to proactively drive value-concordant decision making and monitor the effect on disease control and cost of care.

To cite this abstract in AMA style:
Newman E, Cote J, Chronowski J. Treat to Target Opportunities – Design, Testing, and Adoption of a Novel EHR-Integrated Electronic System to Engage Rheumatologists and Capture Decision Making [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/treat-to-target-opportunities-design-testing-and-adoption-of-a-novel-ehr-integrated-electronic-system-to-engage-rheumatologists-and-capture-decision-making/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/treat-to-target-opportunities-design-testing-and-adoption-of-a-novel-ehr-integrated-electronic-system-to-engage-rheumatologists-and-capture-decision-making/