Session Information
Date: Tuesday, November 12, 2019
Title: 5T098: Orthopedics, Low Back Pain & Rehabilitation (2798–2803)
Session Type: ACR/ARP Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Patients undergoing total knee replacement (TKR) are at increased risk of persistent opioid use and opioid dependence. Group-based trajectory models can identify clusters of patients with clinically distinct, dynamic patterns of medication use over time. Evaluating the characteristics of patients prior to TKR within these empirically identified trajectories of prescription opioid use may be useful in identifying high-risk subgroups.
Methods: Using Medicare Parts A, B and D claims (2010-2014), we identified patients aged ≥65 years who underwent a TKR. All patients were required to be continuously enrolled in Medicare for ≥360 days prior to TKR. To determine opioid filling patterns after TKR, patients were followed up to 360 days from the day of TKR. We modeled 12 monthly indicators of filling as both a continuous (Mean morphine equivalents (MME)/day) variable for Model 1 and a binary (Yes/No for any opioid fill) response variable for Model 2 using censored normal and logistic group-based trajectory models, respectively. Model fit was assessed using a combination of the Bayesian Information Criterion (BIC), predicted probability of group membership and number of patients assigned to each trajectory group. Baseline patient characteristics (assessed in the 360 days prior to TKR) were then tabulated by trajectory group for the final model.
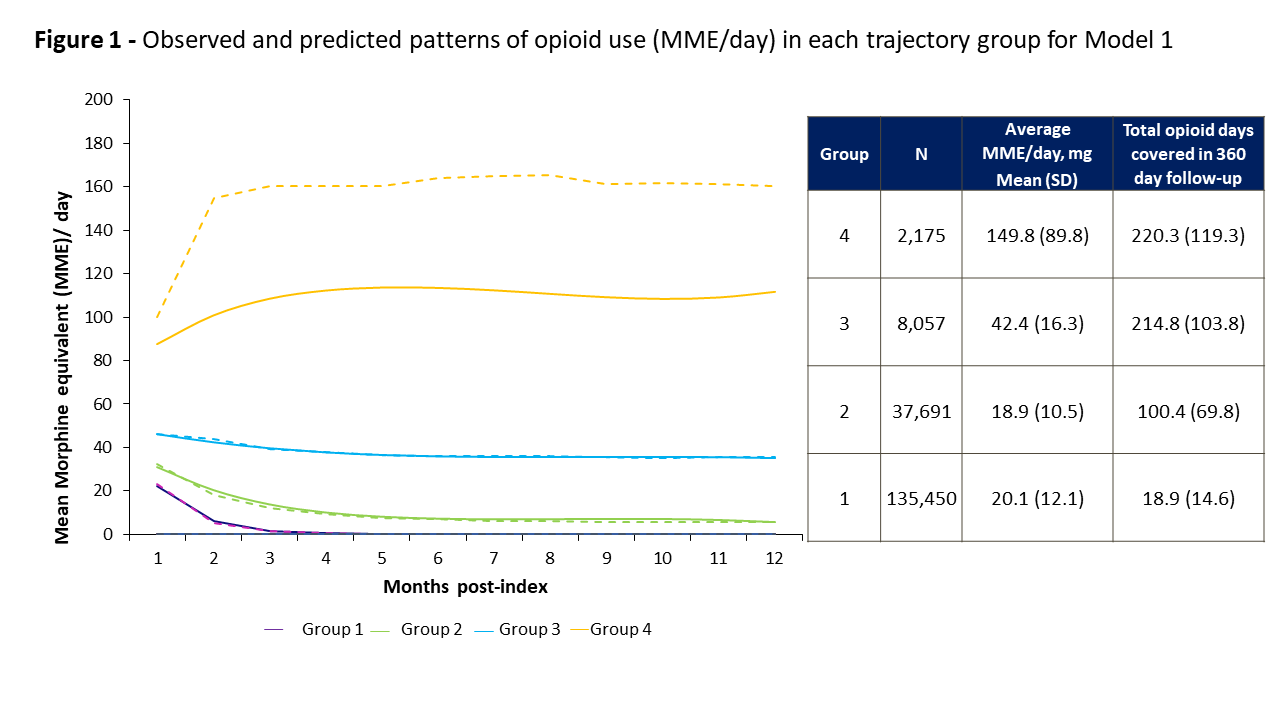
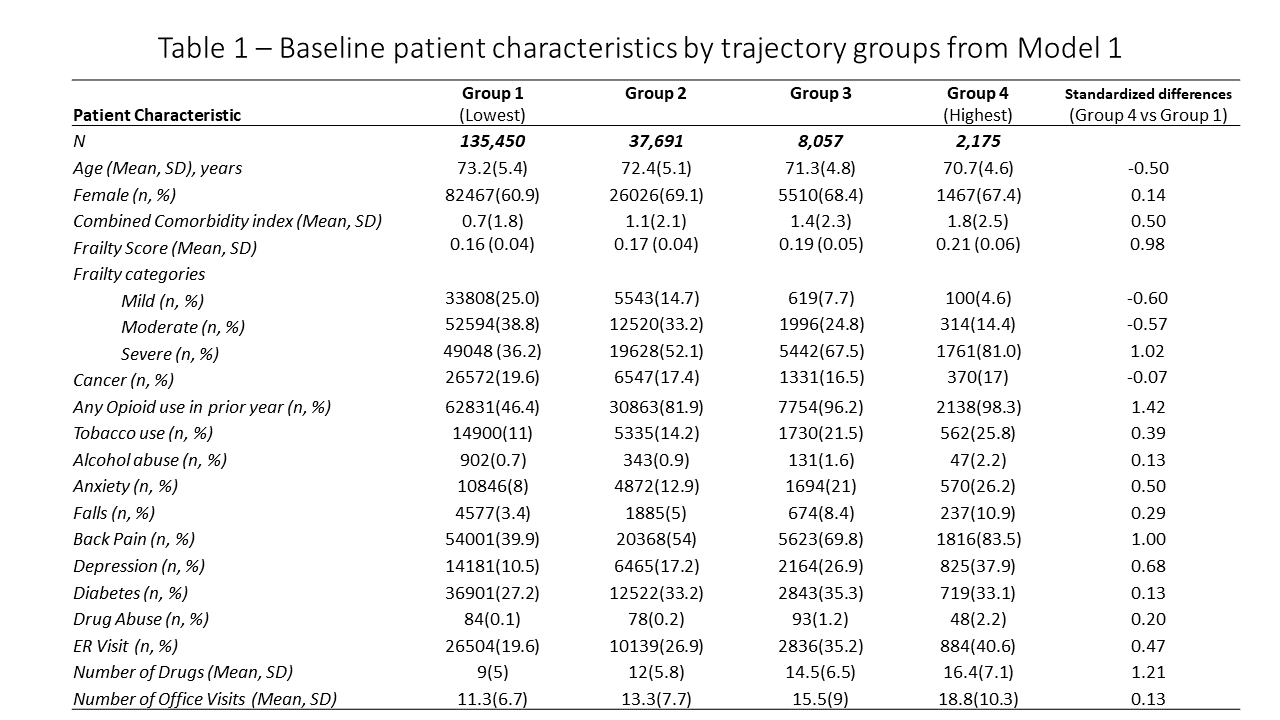
Results: We identified 183,373 patients who underwent TKR during the study period. We selected the 4-group trajectory model as having the best fit for both continuous and binary indicators of filling. Observed and predicted patterns of opioid use in each of the 4 trajectory groups identified by Model 1 are summarized in Figure 1. 78% (n=1,686) of patients assigned to Group 4 (highest opioid use group) from Model 1 were also assigned to Group 4 in Model 2 though the average MME/day in Group 4 was higher (149.8 mg vs. 43.0) in Model 1 compared to Model 2. Hence, Model 1 provided more clinically-meaningful discrimination between patients’ opioid use, and we used trajectory membership based on Model 1 to describe baseline patient characteristics (Table 1). Differences were noted in the baseline characteristics of patients assigned to group 4 compared to those assigned to Group 1 (lowest opioid use). Patients in Group 4 were more likely to be younger, female, have opioid use in the year prior to TKR, and had a greater burden of comorbidities (such as depression, anxiety disorders, back pain), more likely to have used tobacco, alcohol and used more healthcare services in general (number of ER visits, physician office visits and medications used). Patients in Group 4 were also more likely to be frail as assessed by the claims-based frailty index.
Conclusion:
Group-based trajectory models identified a subgroup of patients with high opioid use and whose baseline characteristics prior to TKR were substantially different than those in other groups. Future work could further determine the predictors of persistently high-dose opioid users after TKR and associated adverse events.
To cite this abstract in AMA style:
Gopalakrishnan C, Franklin J, Jin Y, Solomon D, Katz J, Lee Y, Franklin P, Lii J, Desai R, Kim S. Trajectories of Opioid Filling Patterns After Total Knee Replacement [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/trajectories-of-opioid-filling-patterns-after-total-knee-replacement/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/trajectories-of-opioid-filling-patterns-after-total-knee-replacement/