Session Information
Date: Sunday, November 8, 2015
Title: Rheumatoid Arthritis - Small Molecules, Biologics and Gene Therapy Poster I
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Methotrexate (MTX) is standard treatment in
RA. Absorption is better in subcutaneous MTX (scMTX),
which may impact speed of onset. In RA, earlier time to remission
improves long-term results. Objectives were to determine the speed of onset of scMTX with optimal care in early rheumatoid arthritis
(ERA).
Methods: Patients with ERA were studied for outcomes at baseline, 6
weeks and 12 weeks comparing the interval change in DAS28 from 0 to 6 weeks
(early period) and 6 to 12 weeks (late period) to see if more benefit was
observed in very early treatment with scMTX. Repeated
measures ANOVA analyses were performed. The proportion of patients achieving
CDAI, SDAI, DAS28 remission and/or low disease activity across time was
compared.
Results: 103 patients were included from a single site inception
cohort between 2008 to 2014: age 56.2+16.0; 64% female; 57.3% ever-smokers; 59%
RF+; mean disease duration 5.3+3.5 months; 83% met ACR 2010 criteria for
RA. All included patients received MTX (98.0% scMTX,
98% 25mg/week). Few patients reported headache (3%), nausea (4%), and
gastrointestinal symptoms (1.0%), with no dropouts secondary to MTX intolerance
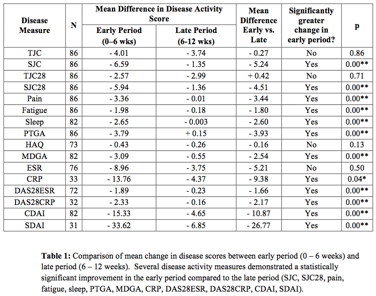
in the first 3 months. The mean change in outcomes between the early and late
time periods are demonstrated in Table 1, with significantly greater change
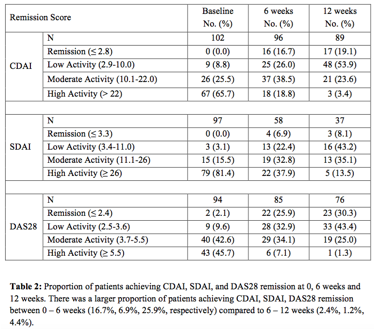
seen in the early period for several outcome measures. There were a larger
proportion of patients achieving SDAI, CDAI and DAS28 remission and/or low
disease activity state in the early versus late period, as shown in Table 2.
There was a significant improvement when using combination DMARD therapy with sc MTX compared to MTX alone at each time point for many
disease measures (TJC, CRP, DAS28, CDAI, SDAI and HAQ), however combination
DMARD cohort size was small (n=9). Co-medication with steroids included 33%
intra-articular, 14% oral, 14% intra-muscular, and 20% combination steroids.
The use of intra-articular steroids with MTX yielded the most disease
measures that improved significantly in the early group (0-6wks) vs. later
(6-12wks).
Conclusion: ScMTX is rapid, as the change in
many disease activity scores was significantly greater between 0-6wks compared
to 6-12wks. The use of combination therapy with DMARDs gave added value
over methotrexate monotherapy, although
generalizability is limited by sample size in the combination cohort.
Intra-articular steroid injections may contribute to the early effect of
treatment in the first six weeks, supporting early effective combination
therapy with scMTX including joint injections as best
practice for rapid improvement.
To cite this abstract in AMA style:
O'Connor A, Thorne JC, Tin D, Pope JE. The Rapid Kinetics of Optimal Treatment with Subcutaneous Methotrexate in Early Inflammatory Arthritis [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/the-rapid-kinetics-of-optimal-treatment-with-subcutaneous-methotrexate-in-early-inflammatory-arthritis/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-rapid-kinetics-of-optimal-treatment-with-subcutaneous-methotrexate-in-early-inflammatory-arthritis/