Session Information
Date: Wednesday, November 11, 2015
Title: Rheumatoid Arthritis - Clinical Aspects VII: Disease Activity and Updates in Measurement
Session Type: ACR Concurrent Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose:
The extent to which a short-term effect of the disease
activity adds to the over-risk of coronary events in patients with Rheumatoid
Arthritis (RA) is largely unknown. Theoretically, inflammation might affect the
vasculature in the long-term by accelerated atherosclerosis, but there have
also been indications of effects on shorter-term risks. For instance,
inflammatory cytokines and inflammation-driven hypercoagulability could affect
the vulnerability of plaques and thrombus formation in the coronaries, i.e.,
processes underlying unstable ischemic heart disease and myocardial
infarctions. In this study we evaluated the risk of acute coronary syndrome
(ACS) shortly after disease activity assessment in a large population of
patients with RA.
Methods:
We assembled all registrations, Jan 1st 2001 to
Dec 31st 2012 from doctor’s visits for patients with a diagnosis of
RA in the Swedish Rheumatology Quality Register (SRQ). The observations were
linked to the Patient Register, the Population Register, and the Cause-of-Death
Register to add information on the outcome (ACS; unstable angina and myocardial
infarction), vital status, emigration, comorbidity (chronic and acute ischemic
heart disease, congestive heart disease, cerebrovascular disease, other
atherosclerotic disease, diabetes, and/or hypertension) antedating the
observation, and socioeconomic factors (educational level, unemployment, sick
leave from work, disability pension). We evaluated the association between
DAS28 and ACS risk in three risk windows (0 to 3, 0 to 6, 0 to 12 months after
each visit, respectively), using three Cox regression models: 1) adjusted for
age, sex and year of visit, 2) additionally adjusted for disease duration,
comorbidity and socioeconomic factors, and 3) adjusted for age and conditioned
on each individual patient, implicitly adjusting for all factors that are
constant within a patient.
Results:
There were 215,135 visits (n patients=31,460, 72.0% women,
mean of age at first visit 59.4 SD 14.5 years) during the study period. The
crude incidence rates were 9.9 (96% CI 9.1-10.9), 10.0 (9.3-10.7), and 10.2
(9.7-10.8) per 1,000 person-years for the 3, 6 and 12 months follow-up,
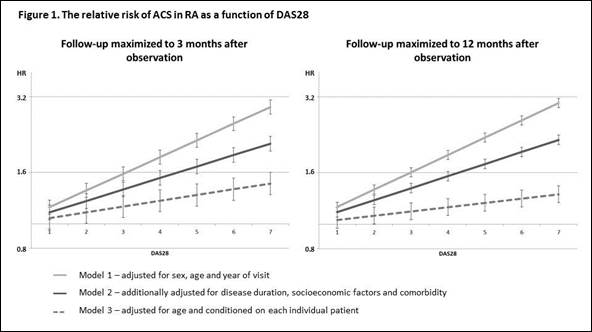
respectively, with 493, 836, and 1203 ACS events occurring during follow-up. Disease
activity score 28-joints (DAS28) was available from 187,659 (87.2%) visits.
DAS28 was associated with the risk of ACS in all risk windows in Models 1 and
2, but the association was weakened in Model 3 (Figure 1). The 12 months follow-up
provided similar results (Figure 1).
Conclusion:
There is a strong link between clinical disease activity and
short-term risk of ACS. Whilst useful for clinical prediction, the association
is, however, only partially likely to be causal, since it was attenuated by
adjustment for socioeconomic factors and comorbidities, in particular when
DAS28 values were compared within each individual.
To cite this abstract in AMA style:
Ljung L, Frisell T, Askling J. The Link Between DAS28 and the Short-Term Risk of Acute Coronary Syndrome in RA, and Its Driving Factors [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/the-link-between-das28-and-the-short-term-risk-of-acute-coronary-syndrome-in-ra-and-its-driving-factors/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/the-link-between-das28-and-the-short-term-risk-of-acute-coronary-syndrome-in-ra-and-its-driving-factors/