Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Pulmonary arterial hypertension (PAH) is the leading cause of systemic sclerosis (SSc) related mortality. We sought to determine survival, predictors of mortality, and health related quality of life (HRQoL) of PAH in a large SSc cohort followed from the time of PAH diagnosis in the modern era of PAH-specific vasodilator therapy.
Methods:
Patients enrolled in a SSc longitudinal cohort between 2009 – 2015 were included. Group 1 PAH was diagnosed on right heart catheterization (RHC) (mPAP ≥25 and PAWP <15 mmHg). Other causes of pulmonary hypertension were excluded. Summary statistics, chi-square tests and survival methods were used to determine survival rates and identify predictors of mortality. HRQoL was measured using the Medical Outcomes Study Short Form 36 (SF-36).
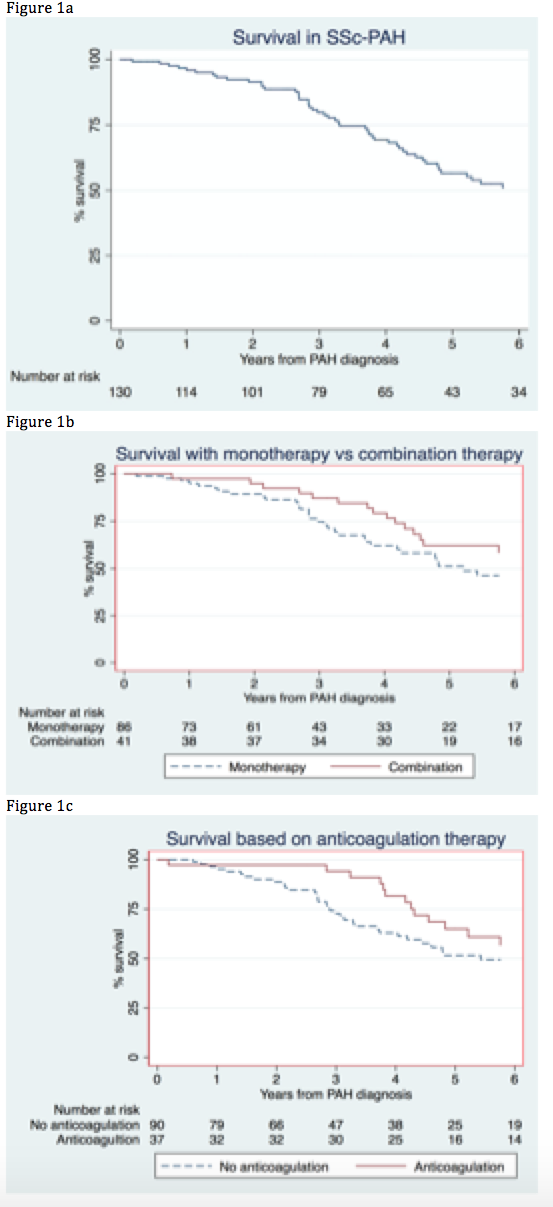
Results: Among 132 SSc-PAH patients, 84.9% were female and 68.9% had limited disease subtype. The mean (±SD) age at diagnosis of PAH was 62.3 (±10.5) years and disease duration at PAH diagnosis was 14.1 (±11.9) years. Over a median (IQR) follow-up of 3.7 (1.6-5.8) years, 60 (45.5%) patients died, with a median survival time from PAH diagnosis of 3.7 years. The standardized mortality ratio for patients with SSc-PAH compared with the general population was 5.8 (95%CI 4.3-7.8). The years of life lost with SSc-PAH was 15.22 years (95%CI 12.3-18.1). Kaplan-Meier survival curves (Figure 1) showed a survival advantage with combination PAH therapy and anticoagulation. Older age at PAH diagnosis (p=0.03), coexistence of mild ILD (p=0.01), worse WHO functional class (p=0.03), higher mean pulmonary arterial pressure at PAH diagnosis (p=0.001) and presence of digital ulcers (p=0.01) during follow-up were predictive of PAH mortality (Table 1). Combination therapy together with anticoagulation provided the most significant survival advantage, with a 72% reduction in mortality compared with pulmonary vasodilator monotherapy without anticoagulation (Figure 1). Patients with SSc-PAH had consistently poorer HRQoL scores in all domains of the SF-36 form except mental health than the general population.
Conclusion: Despite advanced therapy, the median survival in SSc PAH is less than 4 years. The addition of anticoagulation to standard combination therapy is associated with a significant survival advantage, pointing to mechanisms involving endothelial abnormalities and small vessel thrombosis in the pathogenesis of PAH.
|
Table 1. Independent predictors of mortality in SSc-PAH determined by multivariable hazard regression analysis |
||
|
Characteristic |
Hazard Ratio (95% CI) |
p-value |
| Age at diagnosis of PAH, years |
1.05 (1.0-1.1) |
0.03 |
| ILD (FVC > 60%) |
2.83 (1.4-5.6) |
0.01 |
| WHO functional class |
2.01 (1.1-3.9) |
0.03 |
| Pulmonary arterial pressure, mmHg |
1.06 (1.0-1.1) |
0.001 |
| Digital ulcers present |
3.12 (1.4-7.2) |
0.01 |
| Specific PAH therapies and anticoagulation: Vasodilator monotherapy only Vasodilator monotherapy and anticoagulation Vasodilator combination therapy only Vasodilator combination therapy and anticoagulation |
reference 0.39 (0.1-1.2) 0.49 (0.2-1.2) 0.28 (0.1-0.7) |
reference 0.09 0.10 0.007
|
| Abbreviations: PAH pulmonary arterial hypertension, WHO world health organization, ILD interstitial lung disease, 6MWD six minute walk distance, mRAP mean right atrial pressure, mPAP mean pulmonary arterial pressure, HCQ Hydroxychloroquine | ||
Figure 1: Kaplan-Meier survival curves in SSc-PAH
To cite this abstract in AMA style:
Morrisroe K, Huq M, Stevens W, Rabusa C, Sahhar J, Ngian G, Proudman S, Nikpour M. Survival and Health-Related Quality of Life in Incident Systemic Sclerosis Related Pulmonary Arterial Hypertension: A Multicentre Australian Cohort Study [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/survival-and-health-related-quality-of-life-in-incident-systemic-sclerosis-related-pulmonary-arterial-hypertension-a-multicentre-australian-cohort-study/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/survival-and-health-related-quality-of-life-in-incident-systemic-sclerosis-related-pulmonary-arterial-hypertension-a-multicentre-australian-cohort-study/