Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose:
Kawasaki disease (KD) is a systemic medium vessel vasculitis that is predominantly a clinical diagnosis as defined by the American Heart Association (AHA). KD is the most common cause of acquired heart disease in children with 25% of untreated cases developing coronary artery aneurysms (CAAs). Majority of cases occur in children < 5 years of age. In infants, the immune system is immature and classic symptoms of KD are often absent leading to a misdiagnosis or delay in diagnosis. This is the age group where chances of CAA are highest. Complications of CAA include stenosis formation, coronary thrombosis, myocardial infarction, and sudden death. Giant aneurysms have fatal risk of rupture. In this study, we compared clinical profile of infants with giant CAA with those having normal coronaries.
Methods:
This multicentric retrospective study reviewed medical records of 20 infants aged ≤12 months diagnosed with KD managed at Neoclinic Children’s Hospital, Jaipur and Sir Ganga Ram Hospital, New Delhi between April 2019 and June 2025. Demographics, clinical features, laboratory findings, 2D ECHO results, and treatments were documented. Diagnosis was per AHA 2017 criteria, mostly incomplete KD cases. Coronary artery z scores were calculated using Dallaire and Dahdah or Boston formula. Infants were divided into two groups: those with giant coronary artery aneurysms (CAA) and those with normal coronary arteries on ECHO. Data were analyzed using SPSS software. Continuous variables such as age and delay in diagnosis were summarized as medians with ranges and compared using the Mann-Whitney U test. Categorical variables were compared using Fisher’s exact test or Chi-square test where appropriate. A p-value < 0.05 was considered statistically significant.
Results: Among 20 infants, 11 had giant CAAs, and 9 had normal coronary arteries. All infants with giant aneurysms had incomplete KD. Median age at onset was slightly lower at 5 months for giant CAA and 6.5 months for normal group (p=0.12); diagnosis delay was longer in giant CAA group (median 13 vs 10 days, p=0.04). Male predominance was noted in the giant CAA group (73% vs 44% in normal, p=0.37). Common symptoms included fever (100% giant vs 89% normal) and irritability (45% vs 33%). Primary intensification was given in 7/11 (63.6%) giant CAA infants versus none in normal group (p=0.003). IVIG resistance was higher among giant CAA infants (Table 1).
Conclusion: Infants with KD need early identification with aggressive management. Most infants present only with fever and irritability, often leads to delay in diagnoses with high risk for coronary artery abnormalities and long term cardiac sequale.
Younger infants (< 6 months), male sex, delayed treatment initiation beyond 10 days, and abnormal echocardiographic findings at diagnosis are significant predictors for progression to giant aneurysms. Primary intensification of treatment with steroids alongside IVIG may be beneficial in infants at high risk. Close echocardiographic monitoring is essential for timely management. The development of risk scoring systems tailored for the Indian population should be prioritized for better stratification and management of infants with KD.
Infants with giant aneurysms versus normal coronaries 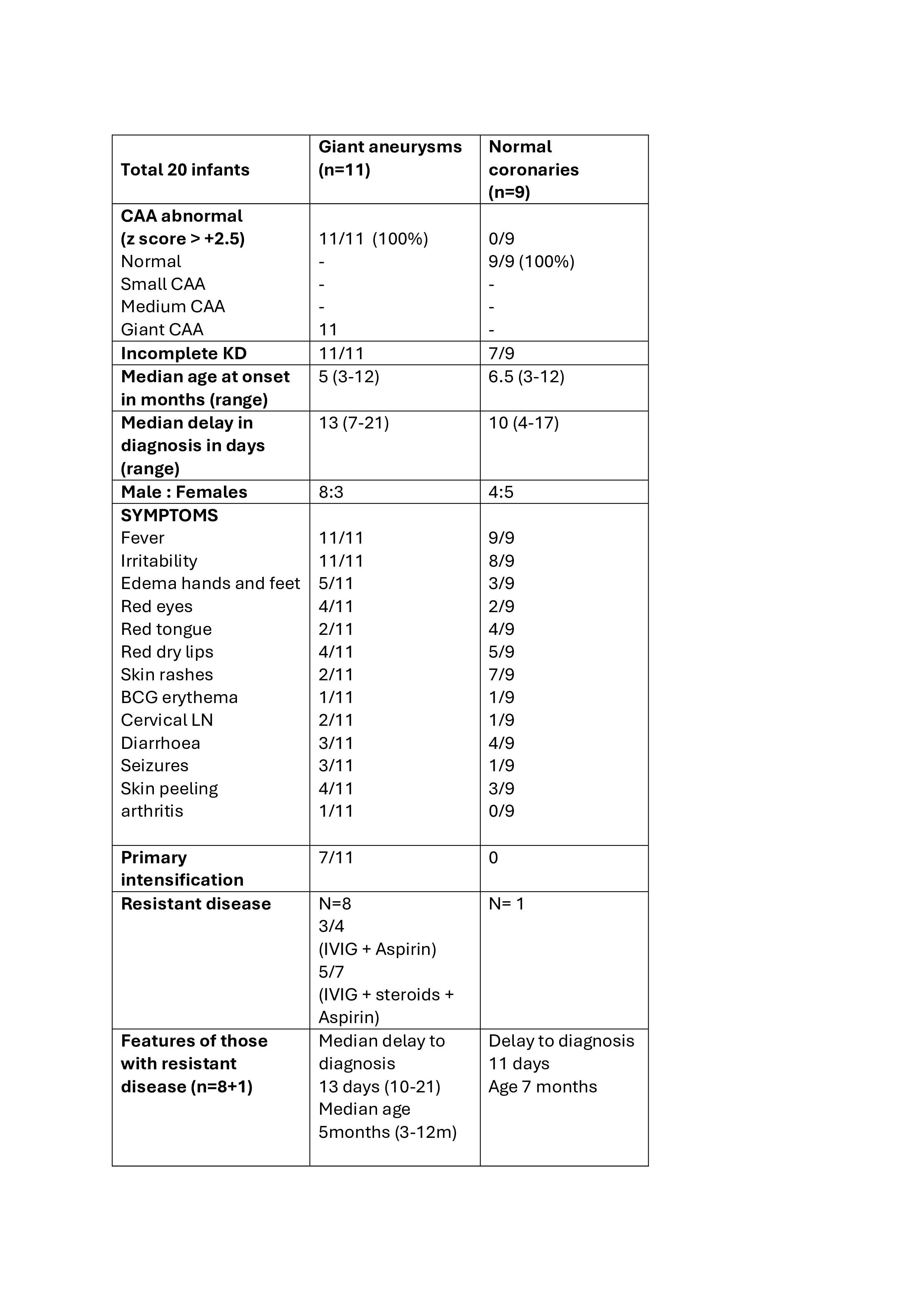
To cite this abstract in AMA style:
Shivpuri A, Agarwal m, Sawhney s. Subtle Signs, Severe Consequences: Clinical profile of infants with giant coronary aneurysms compared to those with normal coronaries. A multicentric retrospective analysis of infants with Kawasaki disease [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/subtle-signs-severe-consequences-clinical-profile-of-infants-with-giant-coronary-aneurysms-compared-to-those-with-normal-coronaries-a-multicentric-retrospective-analysis-of-infants-with-kawasaki-d/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/subtle-signs-severe-consequences-clinical-profile-of-infants-with-giant-coronary-aneurysms-compared-to-those-with-normal-coronaries-a-multicentric-retrospective-analysis-of-infants-with-kawasaki-d/