Session Information
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
|
|
|
|
Background/Purpose: Sclerosis in the sacroiliac joints (SIJ) on radiography and computed tomography (CT) is common but widely considered a non-specific finding of sacroiliitis due to an association with degeneration and osteitis condensans ilii, despite little formal study. Availability of low dose radiation (CT) may lead to more widespread use for diagnostic evaluation. We standardized the definition of sclerosis on CT and then aimed to determine whether this lesion could be reliably detected and its diagnostic utility. |
|
|
Methods: |
|
| 215 CT scans were obtained from patients with a history of low back pain. 107 patients had a clinical diagnosis of spondyloarthritis (SpA) and 108 patients were clinically proven not to have SpA. Both groups were age and gender matched (140 males, 75 females). The mean age was 45 years. Three musculoskeletal radiologists, blinded to patient demographics and diagnosis, scored the CTs after standardization of lesion definitions and calibration. Erosions, sclerosis, and ankylosis were graded by size and number of articular surfaces/ joints involved. Sclerosis was considered definite if located along the cartilaginous compartment, measured >5mm in all 3 planes, and present >5mm from the joint surface. Discrepant scores were arbitrated and inter-reader reliability calculated by intra-class correlation coefficient (ICC). Diagnostic utility of CT lesions was determined by calculating sensitivity and specificity for the clinical diagnosis and by logistic regression. | |
|
Results: |
|
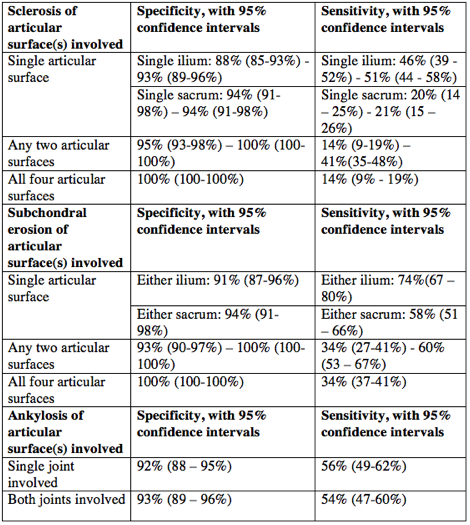
| Inter-observer reliability for scoring sclerosis for each articular surface ranged from 0.65-0.76, 0.71-0.78 for erosion, and 0.87-0.95_ for ankylosis. Sclerosis occurred in 87(81%) cases with SpA and 25 (23%) controls. For a single articular surface the specificity for sacroiliitis ranged between 88-94%, and for any two articular surfaces 95-100%. If all 4 articular surfaces were affected, specificity was 100%. Sensitivity ranged from 14% (4 articular surfaces) to 55% (either ilium). Erosion and ankylosis had a similar specificity range of 91-100% and 92–93%, respectively depending on number of joint surfaces involved. The odds ratio was 4.9 for absence/presence of sclerosis, increasing to 12.55 where there was bilateral joint involvement. For erosion the odds ratio increased to 84.2 for bilateral disease and 22.79 for bilateral ankylosis.
|
|
| Table demonstrating the specificities and sensitivities with 95%CI of subchondral sclerosis, erosion, and ankylosis.
Conclusion: |
|
| When sclerosis measures > 5mm in three planes and is located > 5mm from a joint perimeter, it has high specificity for sacroiliitis, regardless of how many articular surfaces are involved, with similar specificity to erosion. | |
To cite this abstract in AMA style:
Azmat O, Lambert RG, Jibri Z, Maksymowych W. Subchondral Bone Sclerosis on Computed Tomography – Does It Have Any Value in the Diagnosis of Inflammatory Sacroiliitis or Is It a Non-Specific Finding? [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/subchondral-bone-sclerosis-on-computed-tomography-does-it-have-any-value-in-the-diagnosis-of-inflammatory-sacroiliitis-or-is-it-a-non-specific-finding/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/subchondral-bone-sclerosis-on-computed-tomography-does-it-have-any-value-in-the-diagnosis-of-inflammatory-sacroiliitis-or-is-it-a-non-specific-finding/