Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Children with systemic lupus erythematosus (SLE) are at high risk for bone fragility. Studies in pediatric SLE using two-dimensional lumbar spine (LS) dual X-ray absorptiometry (DXA) demonstrate deficits in areal bone mineral density (aBMD). However, the bone structural abnormalities that lead to vertebral compression fractures are unknown. Vertebral volumetric density (vBMD), structure, and compression strength can be estimated using finite element analysis (FEA) of three-dimensional spine quantitative computed tomography (QCT) scans. We performed a cross-sectional study using QCT FEA to assess: 1) LS strength deficits in pediatric SLE and 2) structural determinants of deficits, including vertebral geometry and cortical and trabecular density.
Methods: Participants with SLE were 5-21 years of age and had SLE for at least 1 month. Controls were matched by sex, race (black vs non-black), and Tanner stage. QCT scans of the second lumbar vertebra (L2) were acquired on a Siemens Sensation 64 scanner. FEA strength and density parameters were calculated using VirtuOst 1.2 (ON Diagnostics, Berkeley, CA). DXA scans of L1-4 were obtained using a Hologic QDR 4500A bone densitometer (Apex Software v3.3). Height, body mass index (BMI), fat mass index (FMI), lean mass index (LMI) and LS aBMD Z-scores were generated using reference data from our institution. Multivariable linear regression was used to identify covariates independently associated with L2 strength.
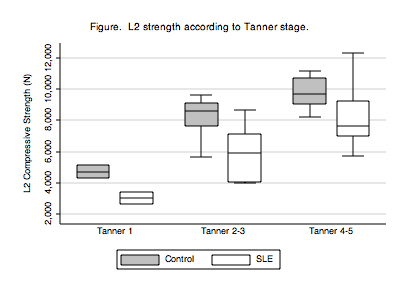
Results: Participants with SLE (n=23, 91% female, 48% black) had a mean age of 14.1 years and significantly lower height Z-scores (-0.05 vs 0.76, p=0.02) and LMI Z-scores (-0.78 vs 0.07, p=0.006). BMI- and FMI Z-scores did not differ between SLE and controls. The median disease duration was 2.1 years (range: 0.3 to 5.8). In SLE, prednisone was prescribed in 74% (median 7.5 mg/day, range: 0-20), hydroxychloroquine in 91%, and immunosuppressants in 74%. LS aBMD Z-scores were lower in SLE (-0.89 vs 0.72, p<0.001). In controls, L2 strength was greater at higher Tanner stages (p≤0.001), adjusting for age and race (both p>0.5). The L2 strength distribution according to SLE and Tanner stage is shown (Figure). In SLE, L2 strength was 21% lower (6844 vs 8688 Newtons (N), p=0.006). The trabecular compartment strength was 26% lower (3659 vs 4913 N, p=0.003), while the cortical compartment strength was 16% lower (3186 vs 3777 N, p=0.04). Further, the inner trabecular vBMD was 18% lower (156 vs 191 mg/cm3, p<0.001), and the cortical vBMD was 9% lower (293 vs 322 mg/cm3, p=0.03). The strength attributable to differences in geometry alone was similar to controls (2643 vs 2840 N, p=0.18).
Conclusion: In the first pediatric study to use vertebral FEA, we found substantial L2 vertebral strength deficits in pediatric SLE. These deficits were not driven by differences in geometry but by the lower cortical and primarily, trabecular bone density.
Disclosure:
J. M. Burnham,
None;
B. S. Zemel,
None;
D. C. Lee,
O.N. Diagnostics, LLC,
3;
T. M. Keaveny,
O.N. Diagnostics,
4,
Amgen, Merck, Wright Medical Tech,
5,
Merck, Lilly, Novartis, Amgen, JandJ,Wright Medic,
2;
M. B. Leonard,
None.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/structural-determinants-of-low-vertebral-strength-in-pediatric-systemic-lupus-erythematosus/