Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: The importance of early, intensive treatment of rheumatoid arthritis (RA) to decrease disease activity and prevent structural damage is established.1 The objective of this analysis was to examine the relationship between disease activity measured by CDAI and DAS28 at week 24, and inhibition of radiographic progression by mean mTSS change from baseline at year 2 in patients treated with etanercept (ETN) + methotrexate (MTX) or MTX monotherapy.
Methods: Randomized subjects from TEMPO (moderate-severe RA, 6.6 years mean disease duration) and COMET (moderate-severe RA, 9 months mean disease duration) who received ETN 50 mg weekly + MTX or MTX alone for 2 years with available X-rays were included in this analysis. Stratified and multivariate regression analyses (observed data) were performed to determine the relationship between variables.
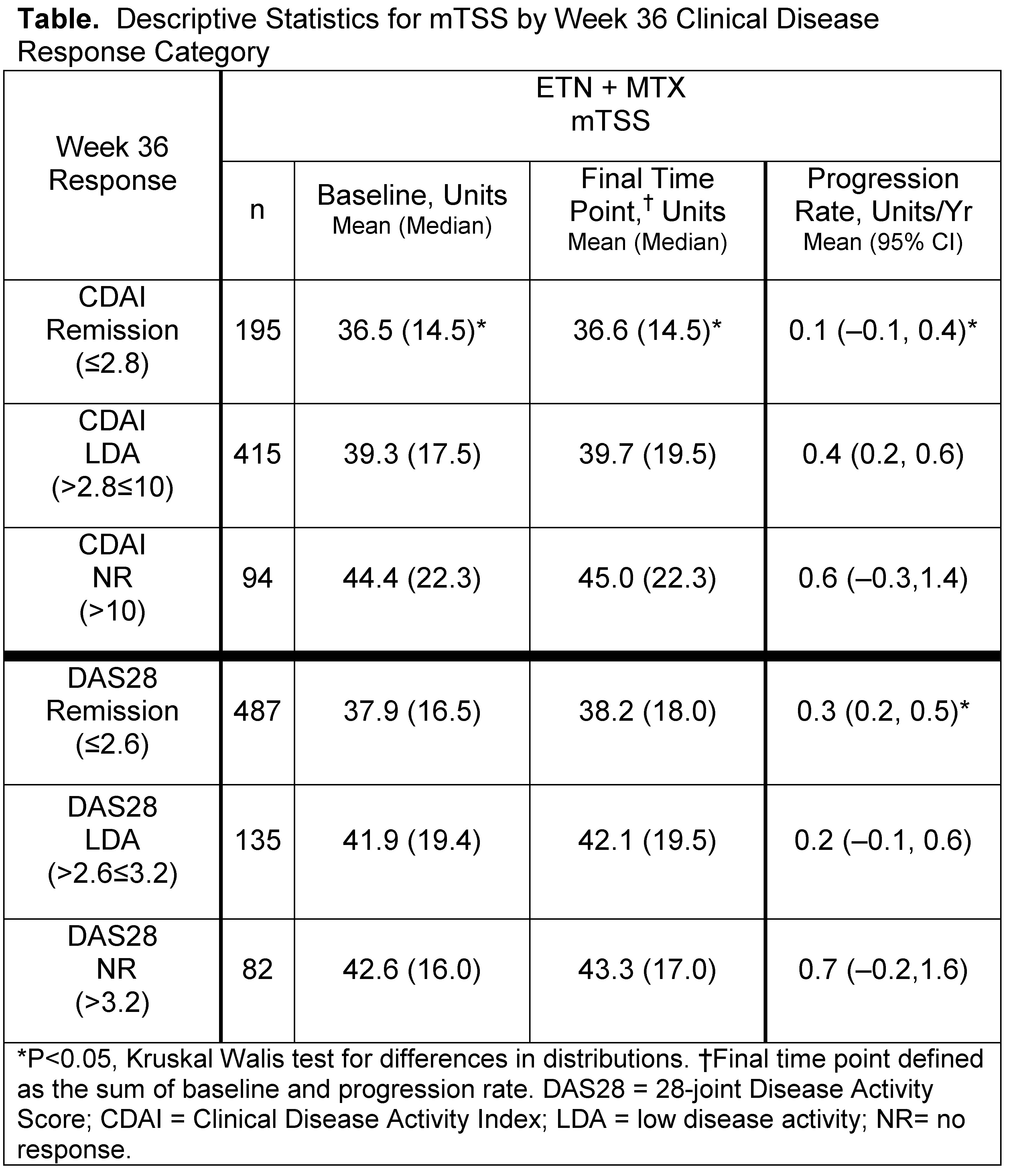
Results: There were a total of 182 patients in COMET and 296 in TEMPO included in this analysis. Patients receiving ETN + MTX had less radiographic progression after 2 years of treatment than MTX monotherapy, independent of disease activity at week 24. In COMET, the percentage of patients achieving CDAI and DAS28 remission in the ETN + MTX group were 17.0% and 46.5% vs 8.8% and 27.7% in the MTX group, respectively. Results were similar in TEMPO with 18.6% and 35.5% of patients in ETN + MTX group and 6.4% and 20.2% in the MTX group achieving remission. Mean change (SD) in annualized mTSS were lower in patients who achieved remission at week 24 compared with those with low disease activity or non-responders, which were significant (P<0.05) in the ETN + MTX group (Table). In the ETN + MTX groups, the majority of patients who achieved CDAI or DAS28 remission were non-progressors by mTSS change scores ≤0.5 (TEMPO 100% and 86.9%; COMET 87.5% and 87.0%) with similar observations in the MTX group (TEMPO 100% and 72.0%; COMET 71.4% and 78.3%).
Conclusion: Inhibition of radiographic progression was more robust with ETN + MTX therapy compared with MTX, regardless of week 24 disease activity. Overall, patients who achieved remission at week 24 had less radiographic progression at year 2 than those with LDA or NR, and less progression with remission defined by CDAI than DAS28. These results may be the first to indicate that achievement of clinical remission within 6 months may predict longer term inhibition of structural damage.
Reference: 1. Combe B. Best Pract Res Clin Rheumatol. 2007;21:1;27–42.
Disclosure:
P. Emery,
Abbott, Merck, Pfizer, UCB, Roche, and BMS,
5;
V. Strand,
Pfizer Inc,
5;
A. S. Koenig,
Pfizer Inc,
3,
Pfizer Inc,
1;
R. Pedersen,
Pfizer Inc,
3,
Pfizer Inc,
1;
E. Bananis,
Pfizer Inc,
1,
Pfizer Inc,
3.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/structural-damage-is-reduced-by-early-achievement-of-clinical-remission/