Session Information
Date: Saturday, November 12, 2022
Title: SLE – Treatment Poster I
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: The efficacy of antimalarials, especially hydroxychloroquine (HCQ), in preventing flares of systemic lupus erythematosus (SLE) is well demonstrated, but its effectiveness is impaired by non-adherence to treatment, reported to vary between 3% and 85%. We aimed to assess the associations of baseline severe non-adherence to HCQ, objectively assessed by HCQ serum levels, and risks of SLE flares, damage, and mortality over 5 years of follow-up.
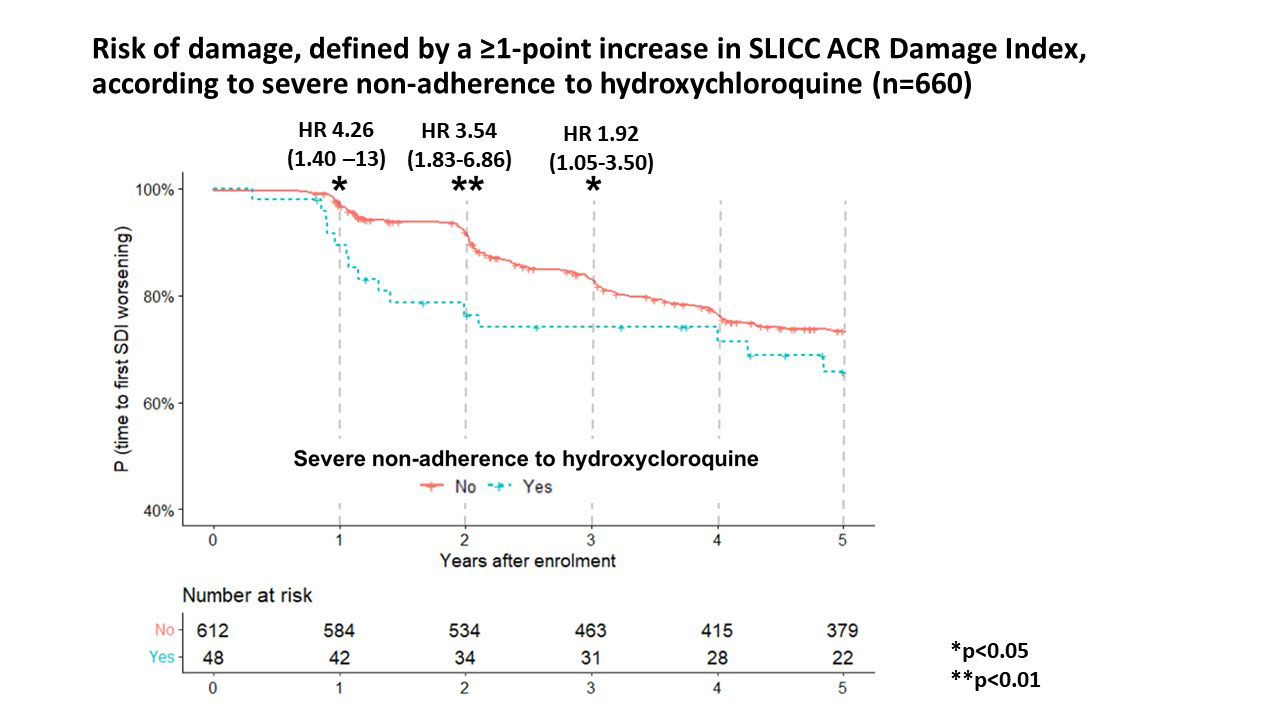
Methods: The SLICC Inception Cohort is a multicentric prospective study of SLE patients from 31 centers in 11 countries. Patients were enrolled within 15 months of recognition of SLE (1997 ACR classification criteria). Serum HCQ levels of patients with HCQ prescription for at least 3 months, sampled at enrollment (or, if unavailable, during the first-year follow-up visits), were centrally measured. Severe non-adherence was defined by a serum HCQ level < 106 ng/mL for a daily prescribed HCQ dose of 400 mg, and < 53 ng/mL for a daily HCQ dose of 200 mg, respectively (1). SLE flare was defined by the occurrence of one of the following events within the first year following serum collection: (a) increase of at least four point in the SLEDAI-2K; (b) new start in prednisone (oral or pulse) or immunosuppressive agent; (c) a new renal involvement (active nephritis, nephrotic syndrome). Association between severe non-adherence and SLE flare was assessed with logistic regression models, further adjusted on potential confounders. Damage was assessed by the time until an increase ≥1 in the SLICC damage index (SDI), within the 5 years following HCQ measurement. Associations between severe non-adherence and either damage or mortality (from all cause) within 5 years following HCQ measurement were assessed with Cox proportional hazard models, adjusted on sex, education, and potential confounders.
Results: Of 1849 cohort subjects, 660 patients (88% women) were included. Median [interquartile range] serum HCQ level was 388 ng/mL (244-566) and 48 patients (7.3%) had severe HCQ non-adherence. No factors were clearly associated with severe non-adherence. A SLE flare occurred in 191 (28.9%) patients within the first year (28 [58.3%] non-adherent patients versus 163 [26.6%] other patients). In multivariate analysis, severe nonadherence was independently associated with the risk of flare (OR= 3.32; 95% CI 1.78-6.28).
Within five years, 167 patients (25.3%) had ≥1 point increase of SDI. Severe on-adherence was associated with an increase in the SDI within each of the first 3 years (HR 1.92 at 3 years; 95% CI 1.05–3.50).
Eleven patients died within 5 years, including 3 with severe non-adherence (unadjusted HR 5.41; 95% CI 1.43–20.39).
Conclusion: In this large multicentric international prospective cohort, severe non-adherence was independently associated with the risk of SLE flare in the following year, with early damage, and 5-year mortality. As severe non-adherence is often unknown by the physician and since no predictive clinical or biological factors were identified, our results suggest the benefits of testing to detect severe non-adherence, to identify the patients at risk.
To cite this abstract in AMA style:
Nguyen Y, BLanchet B, Urowitz M, Hanly J, Gordon C, Bae S, Romero-Diaz J, Sanchez-Guerrero J, Clarke A, Bernatsky S, Wallace D, Isenberg D, Rahman A, Merrill J, Fortin P, Gladman D, Bruce I, Petri M, Ginzler E, Dooley M, Ramsey-Goldman R, Manzi S, Jönsen A, Alarcón G, van Vollenhoven R, Aranow C, Le Guern V, Mackay M, Ruiz-Irastorza G, Lim S, Inanc M, Kalunian K, Jacobsen S, Peschken C, Kamen D, Askanase A, Buyon J, Costedoat-Chalumeau N. Severe Non-adherence to Hydroxychloroquine Is Associated with Flares, Early Damage, and Mortality in Systemic Lupus Erythematosus: Data from 660 Patients from the Systemic Lupus International Collaborating Clinics (SLICC) Inception Cohort [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/severe-non-adherence-to-hydroxychloroquine-is-associated-with-flares-early-damage-and-mortality-in-systemic-lupus-erythematosus-data-from-660-patients-from-the-systemic-lupus-international-collabor/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/severe-non-adherence-to-hydroxychloroquine-is-associated-with-flares-early-damage-and-mortality-in-systemic-lupus-erythematosus-data-from-660-patients-from-the-systemic-lupus-international-collabor/