Session Information
Session Type: Poster Session (Sunday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Cardiac sarcoidosis (CS) is a rare, life-threatening disease and the second leading cause of death in patients with sarcoidosis. Currently, the recommended treatment for CS includes corticosteroids, optimal heart failure therapy, arrhythmia management, and prevention of heart block complications. The role of steroid sparing agents in the treatment of CS is not well described. Our aim was to review the clinical characteristics and treatment modalities of CS in our center and analyze patient outcomes who received oral immunosuppressive agents or a Tumor Necrosis Factor-alpha inhibitor (TNFi) as a part of their CS management.
Methods: We performed a retrospective chart review of all patients diagnosed with sarcoidosis from 2014 to 2019 at Loma Linda Medical Center. Patients that were diagnosed with CS (as defined by the Heart Rhythm Society diagnostic criteria) were included in the analysis.
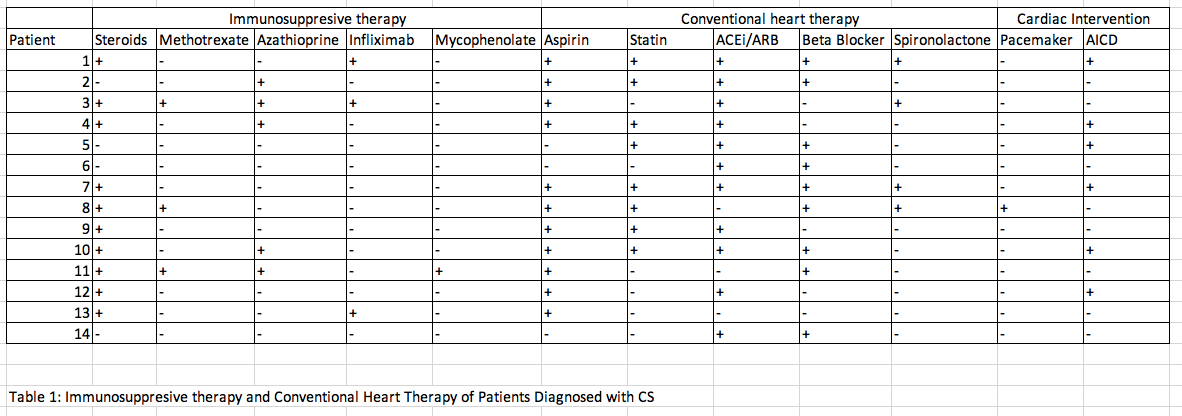
Results: Out of 496 patients who have been diagnosed with sarcoidosis, 14 patients were diagnosed with CS in accordance with the Heart Rhythm Society guidelines. The average age was 58, 2:5 male to female ratio, and an average body mass index of 30.3. Seventy one percent of patients had biopsy proven sarcoidosis and the remaining 29% were diagnosed by clinical and imaging criteria. The most common presenting cardiac manifestation was new onset heart failure (64%), followed by cardiac arrhythmias (46%) of which more than half of patients presented with AV blocks (29%). All patients except one were initially diagnosed with sarcoidosis involving other organs (lungs (71%), skin (28%), lymph node (28%) joints (14%), GI tract manifestation (21%), neurological manifestations (21%). Cardiac manifestation was the initial presenting symptomatology of sarcoidosis in one patient. The average duration between initial diagnosis of sarcoidosis until diagnosis of CS was 5 years. The average duration between initial cardiac symptom onset and CS diagnosis was 4 years. Abnormal findings were noted on echocardiography (46%), cardiac magnetic resonance imaging (46%) noted as patchy myocardial scar, myocardial late gadolinium enhancement and positron emission tomography scan (40%). Patients were treated with corticosteroids (78%), azathioprine (36%), methotrexate (14%), infliximab (21%), mycophenolate (7%), hydroxychloroquine (7%), adalimumab (14%), cyclophosphamide (14%), and tacrolimus (7%) in addition to their conventional heart therapy. (Table 1). Three patients did not undergo any treatment for CS given their subclinical/asymptomatic status. Six of the analyzed patients had echocardiogram after initiation of immunosuppressive therapy. All patients except for one demonstrated either improvement, or no worsening of their left ventricular ejection fraction (LVEF) (table 1). One patient showed worsening of the LVEF due to noncompliance.
Conclusion: There are no formal guidelines for management of CS. We describe clinical manifestations and treatment outcomes of 14 patients with CS managed with an oral immunosuppressive agent or TNFi with favorable outcomes. Further larger scale prospective studies are required to identify the most appropriate immunosuppressant regimen and conclude its efficacy in management of CS.
To cite this abstract in AMA style:
Injean P, Lee Y, Hojjati M. Role of Alternative Immunosuppressant Therapy in Management of Cardiac Sarcoidosis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/role-of-alternative-immunosuppressant-therapy-in-management-of-cardiac-sarcoidosis/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/role-of-alternative-immunosuppressant-therapy-in-management-of-cardiac-sarcoidosis/