Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Progression of joint damage is sometimes observed in JIA patients during the biologic therapy. However, it is difficult to evaluate the radiographic progression by simple radiographs because the width of joint space and ossification varies with age. Carpal length (CL) is a useful measure component for identifying joint space narrowing due to cartilage damage of the wrist in children1-2).
Therefore, the risk factors for radiologic progression during the biologic therapy were investigated by evaluating the CL in polyarticular JIA patients.
Methods: Forty-six polyarticular JIA patients initiating biologics were followed up prospectively for mean 3.1 years. RF was positive in 36 out of 46, and all had active arthritis in the wrist at starting biologic therapy. Duration from the onset to initiating biologics was mean 3.1 years, and the 1st biologic agents used were etanercept in 21, adalimumab in 7, infliximab in 9, and tocilizumab in 9. CL was measured from radiographs of the wrist obtained at baseline (n=46), at 1year (n=36), and at 3 year (n=20), and the standard deviation (SD) of CL calculated by Poznanski’s formula established from healthy children1) was analyzed.
Results:
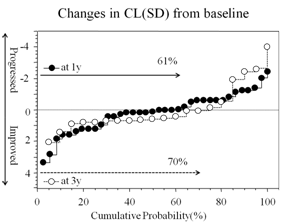 1) Changes in CL (SD) from baseline (Figure)
1) Changes in CL (SD) from baseline (Figure)
At 1 year after starting biologics, incidence of patients with increased (improved) or sustained CL(SD) was 61%, which indicated that 61% patients had no radiographic progression of joint damage of the wrist during the first year of biologic therapy. At 3 year from baseline, 70% of patients showed no radiographic progression of joint damage.
2) Risk factors for progression of joint damage.
Background, clinical features, disease activity by DAS28ESR, and the biologic therapy were compared between two groups of patients with improved/sustained CL(SD) and with non-improved CL(SD) to determine the risk factors for radiologic progression after 1 year biologic therapy.
As the result, incidence of the patients showed no statistical difference between the two groups as to sex (male, female), onset age (<10 y, ≥10 y), RF (positive, negative), disease duration at initiating biologic therapy (<1 y, 1-<3 y, ≥3 y), 1st biologic agent used, and episode of switching to the 2nd biologic agent. However, the incidence of patients who attained DAS28<2.6 remission was significantly higher in improved/sustained CL(SD) group (100%) than that of non-improved CL(SD) group (46%) (Qui square=7.038, P=0.0080).
Conclusion:
Biologics can prevent the radiologic progression of wrist in only patients who attained the DAS28<2.6 remission during the first year treatment. Switching to the 2nd biologic agent may be needed in polyarticular JIA patients who failed to complete the DAS28<2.6 remission.
1) Poznanski AK et al. Radiology 1978;129:661-8. 2) Ravelli A, et al. J Pediatr 1998; 133:262-5
Disclosure:
T. Kubota,
None;
T. Yamatou,
None;
Y. Nonaka,
None;
H. Akaike,
None;
T. Nagakura,
None;
Y. Yamasaki,
None;
T. Takezaki,
None;
Y. Nerome,
None;
H. Imanaka,
None;
S. Takei,
Chugai, Eisai, Takeda, Brystol-Mayers Japan,
2.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/risk-factors-for-radiologic-progression-in-polyarticular-juvenile-idiopathic-arthritis-patients-treated-with-biologic-agents/