Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Micronutrient deficiencies can lead to protean clinical manifestations, including those mimicking autoimmune or auto-inflammatory diseases, contributing to misdiagnosis, delay in treatment, and even unnecessary immunosuppression. Individuals with restrictive eating behaviors, developmental disorders, or malabsorption are particularly vulnerable. We present three children and one young adult where the phenotypes prompted extensive evaluation before underlying nutritional deficiencies were identified.
Methods: A review of sequential patient records of children and young adults diagnosed with nutritional deficiency mimicking rheumatic disease was conducted in Albany Med Health System.
Results: The demographic parameters, clinical features, clinical progress with initial treatments, key lab and imaging findings and outcome of the cases are summarized in the Table (Figure 1)
Conclusion: These cases highlight the need to recognize severe nutritional deficiencies as mimics of rheumatic diseases. The first case demonstrates how vitamin C deficiency could resemble lupus, vasculitis, Inflammatory bowel disease and chronic nonbacterial osteomyelitis. The second case is a rare combination of scurvy and rickets raising concerns for leukocytoclastic vasculitis, arthritis and even musculoskeletal manifestations of acute leukemia. The third patient is a young adult who underwent extensive and invasive work-up before being treated for avoidant restrictive food intake disorder (AFRID)-a diagnosis that was unmasked by its complication of scurvy mimicking a vasculitic rash. Lastly, in the fourth case, pachymeningitis with progressive visual loss raised suspicions for Behcet’s disease, neurosarcoid and IgG4 related disease but was ultimately found to be due to vitamin deficiencies. These cases underscore the importance of a detailed dietary history and full nutritional assessment, especially in at-risk individuals in preventing misdiagnosis, unnecessary immunosuppression, and treatment delay
Table: Demography, Clinical Presentation, Lab and Imaging Data, Rheumatology Mimics, Final Diagnosis and Underlying Risk Factors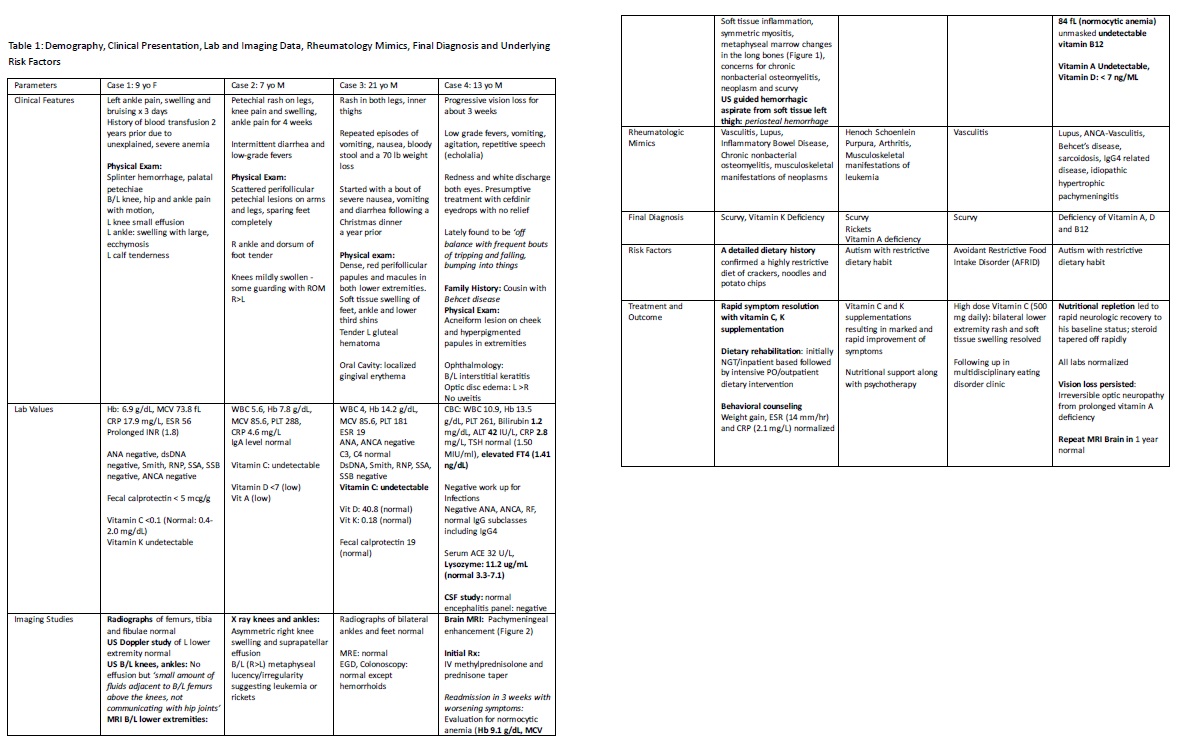
MRI B/L lower extremities (Case 1)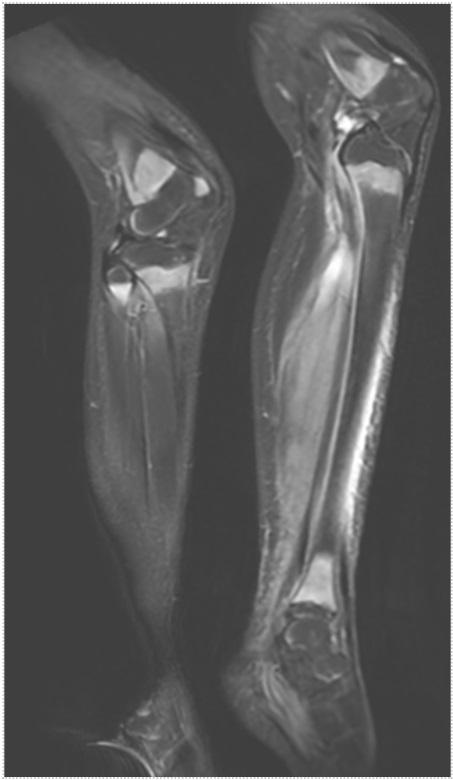 Case 1: MRI Oblique coronal short tau inversion recovery (STIR) image of the bilateral lower extremities demonstrates symmetric T2 hyperintensity in the bilateral distal femoral metaphysis, as well as the proximal and distal tibial metaphysis
Case 1: MRI Oblique coronal short tau inversion recovery (STIR) image of the bilateral lower extremities demonstrates symmetric T2 hyperintensity in the bilateral distal femoral metaphysis, as well as the proximal and distal tibial metaphysis
MRI Brain (Case 4)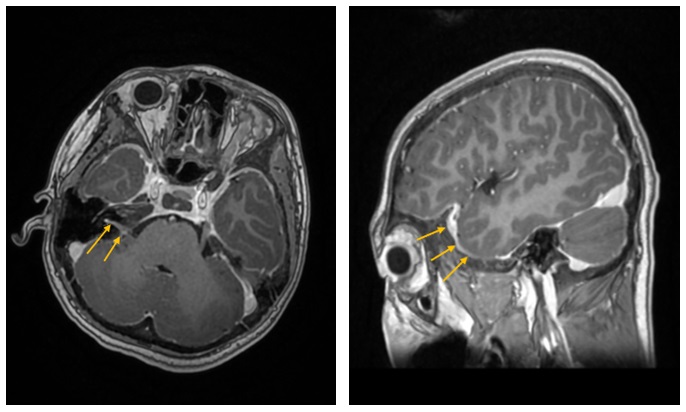 Case 4: MRI brain showing mild diffuse pachy-meningeal enhancement, pituitary hypo-enhancement (normal functional studies), possible neuritis of the auditory canals and prominence of the optic discs bilaterally
Case 4: MRI brain showing mild diffuse pachy-meningeal enhancement, pituitary hypo-enhancement (normal functional studies), possible neuritis of the auditory canals and prominence of the optic discs bilaterally
To cite this abstract in AMA style:
Maharjan H, Ostrov B, Kong E, Ganguli S. Rheum2Fake: Lessons from Severe Nutritional Deficiencies [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/rheum2fake-lessons-from-severe-nutritional-deficiencies/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/rheum2fake-lessons-from-severe-nutritional-deficiencies/