Session Information
Date: Sunday, November 13, 2016
Title: Imaging of Rheumatic Diseases - Poster I: Ultrasound and Emerging Technologies
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
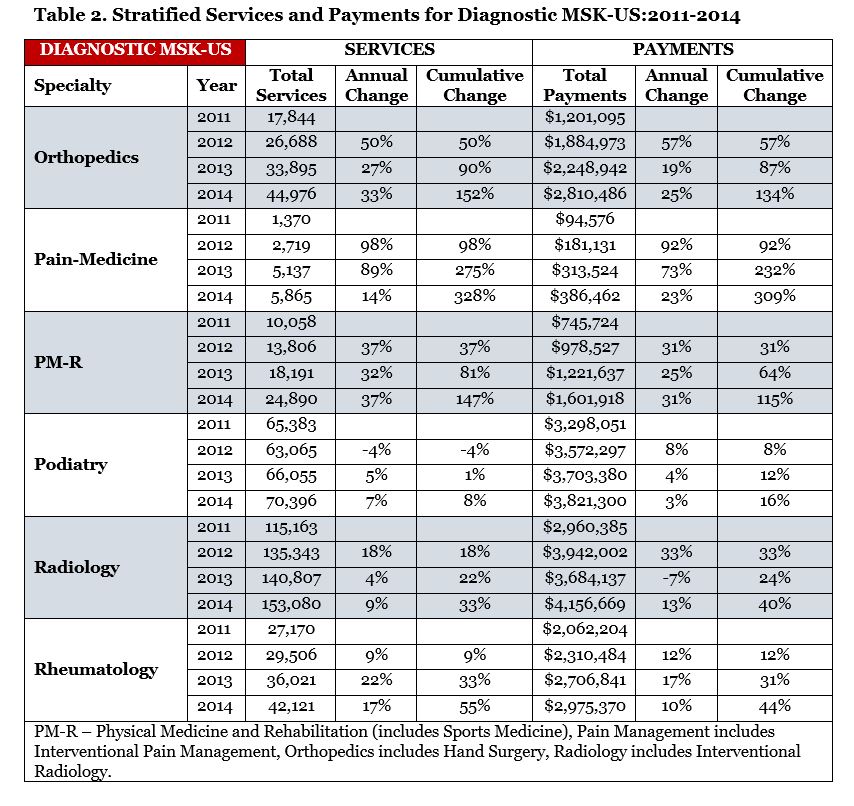
Background/Purpose: Rapid rise in the use of diagnostic and interventional MSK-US within the Medicare population between 2011 and 2013 has been documented amongst non-radiology MSK providers.1 Due to rapid escalation of cost and utilization, Medicare recently identified interventional MSK-US CPT 76942 as a potentially incorrectly estimated code leading to the reported payment reductions.2 The key objective of this study was to determine the four-year trend of utilization of diagnostic and interventional MSK-US using the recently available 2014 Medicare Part B data. The secondary objective was to assess the impact of CPT 76942 code revaluation by Medicare.
Methods: A retrospective secondary analysis of Medicare Physician Supplier Payment Summary (PSPS) files from 2011 – 2014 was used to describe the services and total payments on utilization of MSK-US. PSPS data is aggregated on multiple factors with certain exclusions, including absence of technical costs such as those billed by Radiology. Therefore, service count data more accurately reflects utilization across specialties. CPT 76881, 76882 and 76942 were coded as diagnostic MSK-US and interventional MSK-US respectively. Non-duplicative billing claims of these codes were summed for each years and provider specialty. MSK provider specialties were also grouped into six groups. Descriptive analysis was conducted using R-Studio (Version 0.98.1102) and Tableau (Version 9.3).
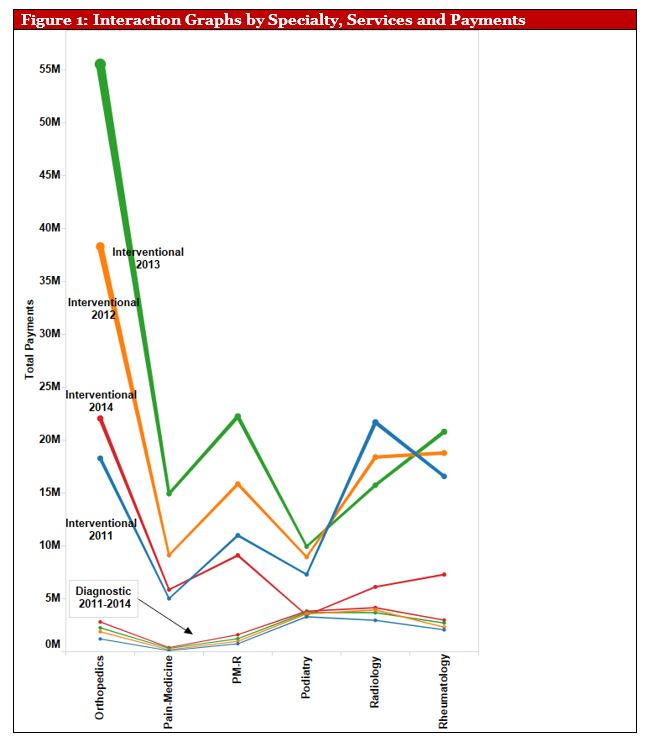
Results: Interventional MSK-US services continued to grow in most specialties except for Radiology where they continued to decline every year (Table 1). Orthopedics continued to rank the highest for interventional MSK-US services, whereas Rheumatologists’ services remained fairly stable with a minor reduction from 2013 to 2014. Strikingly, there was a 60-65% cut in payments in 2014 (Figure 1). There continued to be a greater utilization of interventional than diagnostic MSK-US among all MSK providers except Podiatry (Table 1 and 2).
Conclusion: A marked dissociation of interventional MSK-US services from diagnostic services continued to be seen in most MSK specialties. The radical cut in payments is notable not only due to its magnitude but also that it pre-dated bundled billing of common joint injections with MSK-US. The next logical step for future research will be to assess and correlate the reduction in the observed payment with the reduction of interventional MSK-US. 1. Kaeley GS, Kraemer D, Smotherman C, Dodani S. Musculoskeletal Ultrasound (MSK-US): Innovation or Overutilization? Arthritis Rheumatol. 2015;67.
2. 2014-Medicare-Physician-Fee-Schedule-Final-Rule. 2014

To cite this abstract in AMA style:
Kaeley GS, Dodani S. Reduction in Musculoskeletal Ultrasound (MSK-US) Payments in 2014: Effects & Consequences [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/reduction-in-musculoskeletal-ultrasound-msk-us-payments-in-2014-effects-consequences/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/reduction-in-musculoskeletal-ultrasound-msk-us-payments-in-2014-effects-consequences/