Session Information
Date: Tuesday, November 14, 2023
Title: (2257–2325) SLE – Diagnosis, Manifestations, & Outcomes Poster III
Session Type: Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Infections are a major cause of morbidity and mortality in systemic lupus erythematosus (SLE). We studied whether infections cluster together and which patients are susceptible to recurrent infections.
Methods: Adult and juvenile SLE (ACR 1997 criteria) from 2000-2020 were reviewed retrospectively for minor and serious infections. Clusters were determined by principal coordinate analysis of a distance matrix from a random forest model.
Results: Of 1576 patients(1452 Female, mean age 27.98±10.53 years) with 8281.34 person-years of follow-up, 663 infections occurred in 490 individuals. Gram-negative bacteria were the most common, followed by mycobacteria (Table 1).
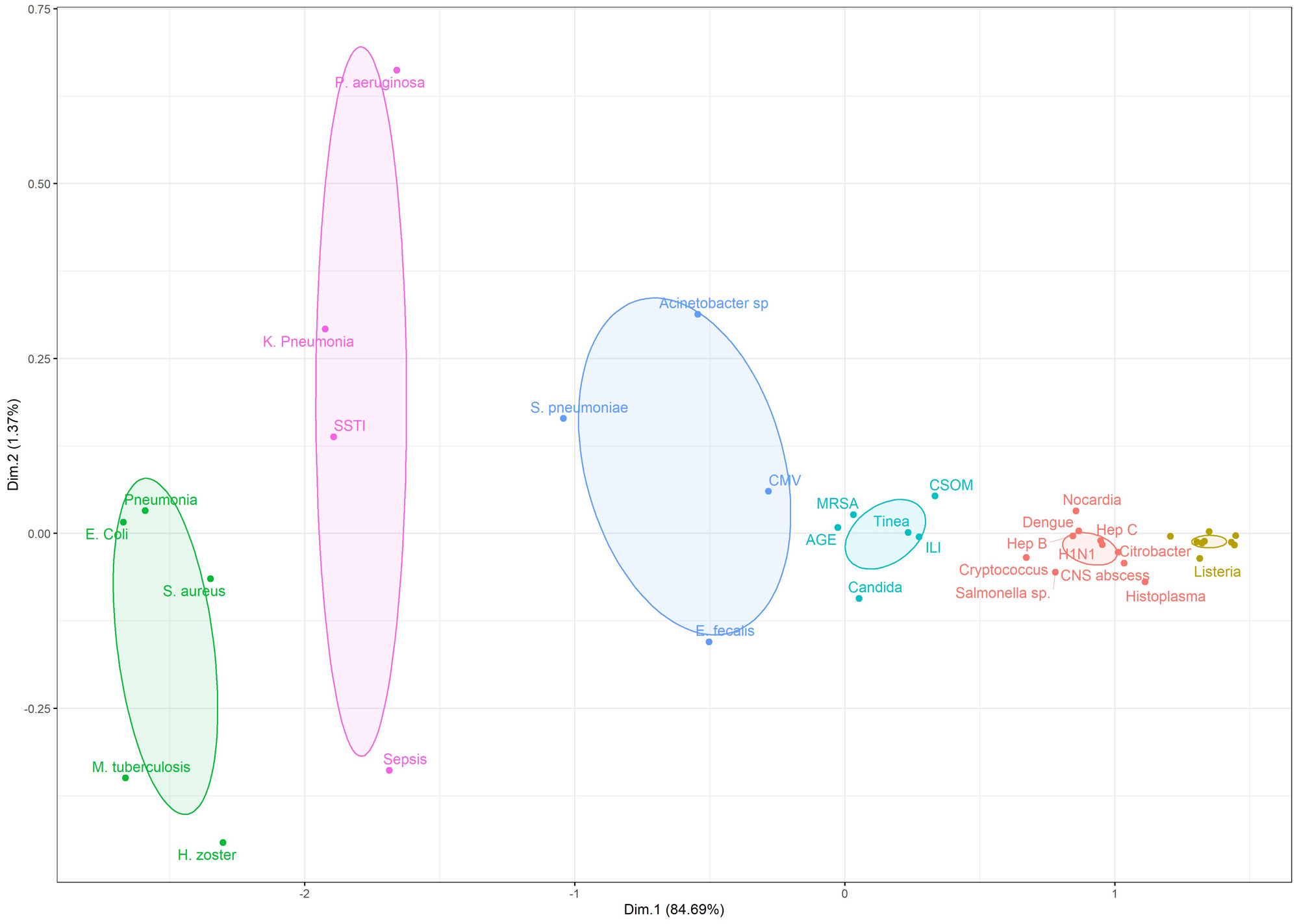
We identified 3 major and 3 minor clusters(Figure 1). Cluster 1 included predominantly intracellular infections: M. tuberculosis, S.aureus, H.zoster, E.coli, and pneumonia(microbiologically unconfirmed). Cluster 2 included bacterial infections: P.aeruginosa, K.pneumoniae, soft tissue infection, and sepsis(microbiologically unconfirmed). Cluster 3 included S.pneumoniae, E.fecalis, Acinetobacter, and Cytomegalovirus.
Cluster 1 was associated with fever(OR 1.95,1.39-2.73), nephritis(OR 1.6,1.23-2.06), myositis and serositis(OR 1.51,1.10-2.06), higher SLE disease activity index (SLEDAI) (14 vs 10), anti dsDNA(192 vs 150), low absolute lymphocyte counts(1296 vs 1512/cumm), C3(52.5 vs 61.8 mg/dl) and albumin(3 vs 3.5 g/dl). Cluster 2 was associated with nephritis(OR 2.02, 1.33-3.06), gastrointestinal manifestations(OR 2.76, 1.13-6.75) and antiphospholipid syndrome(OR 1.87, 1.03-3.39), higher SLEDAI(14 vs 11), higher anti dsDNA antibodies(200 vs 150), low total leukocyte counts(5750 vs 6400) with similar absolute lymphocyte counts(1368 vs 1476), low C3(51.8 vs 61) and albumin(3.1 vs 3.5 g/dl). Cluster 3 was associated with low total leucocyte count(5100 vs 6400) and similar lymphocyte counts(1181 vs 1470), low C3(43.5 vs 60 mg/dl), and albumin(2.8 vs 3.4 g/dl).
Conclusion: A subset of patients prone to intracellular infections have lower lymphocytes. Patients prone to bacterial infections have lower total leukocyte counts with similar lymphocytes suggesting neutrophil deficiency. We hypothesize that functional assay of these cell lines in may predict future infection risk.

To cite this abstract in AMA style:
Chatterjee R, Pattanaik S, Misra D, Agarwal V, Lawrence A, Misra R, Aggarwal A. Recurrent Intracellular Infections Cluster Together in Patients of SLE with Lymphopenia and Active Disease [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/recurrent-intracellular-infections-cluster-together-in-patients-of-sle-with-lymphopenia-and-active-disease/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/recurrent-intracellular-infections-cluster-together-in-patients-of-sle-with-lymphopenia-and-active-disease/