Session Information
Date: Sunday, October 21, 2018
Title: Muscle Biology, Myositis and Myopathies Poster I: Clinical Features and Disease Course
Session Type: ACR Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Clinical manifestations of
Methods: We conducted a retrospective chart review of patients with ASS with Jo-1, PL-7, PL-12, EJ and OJ antibodies between 2003 – 2017. ASS patients with PH were selected for further review. PH was diagnosed by right heart catheterization (RHC) in all patients with mean pulmonary arterial pressure (mPAP) ≥25
Results: We identified 177 patients with
Conclusion: PH is not uncommon in patients with ASS. 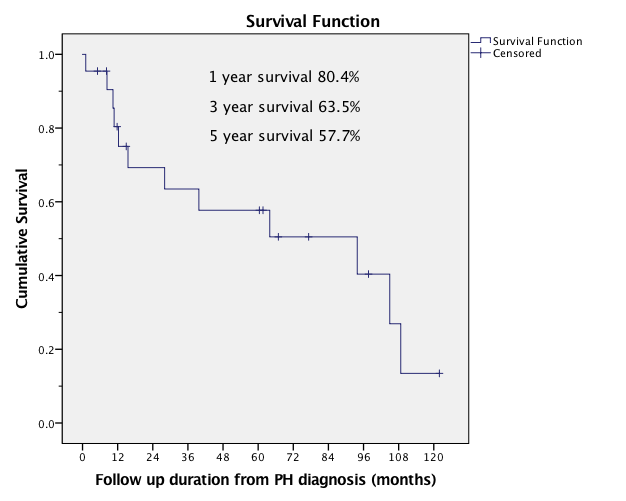
To cite this abstract in AMA style:
Carneiro C, O-Charoen P, Chatterjee S. Pulmonary Hypertension in Anti-Synthetase Syndrome [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/pulmonary-hypertension-in-anti-synthetase-syndrome/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/pulmonary-hypertension-in-anti-synthetase-syndrome/