Session Information
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Rituximab (RTX) is effective for maintaining remission in ANCA-associated vasculitis (AAV) but increases risks for vaccine-preventable severe infections and reduces the immune response to vaccination. There is uncertainty regarding risks and benefits of holding RTX to improve vaccine efficacy by permitting B cell repopulation (e.g., seasonal flu, COVID-19). We used the previously validated microsimulation model, AAV-Sim, to project the clinical impact of delaying treatment with RTX in people with AAV in remission.
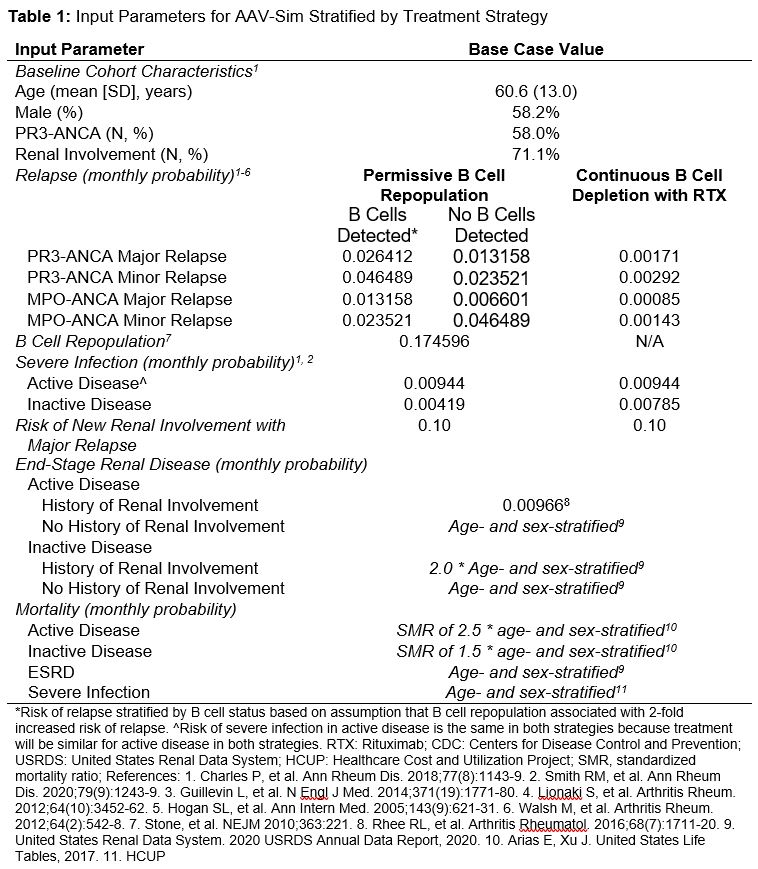
Methods: We evaluated 2 strategies: (1) Continuous B cell depletion with routine RTX retreatment; or (2) Permissive B cell repopulation with RTX delayed for 4 weeks to optimize vaccination, then resuming RTX. At model start, individuals are in remission, B cell depleted, and have an eGFR ≥45ml/min. They are assigned demographics, ANCA type, and other characteristics based on probabilities, and transition monthly between active (e.g., major/minor relapse) or inactive AAV states. They are monitored monthly for B cell repopulation and are at risk for severe infection, end-stage renal disease (ESRD), or death. Transition rates are stratified by demographic and disease-specific characteristics (Table 1). We projected the primary outcomes of relapse-free remission and vaccine optimization over 12 months. We defined vaccine optimization as: B cell repopulated, retreatment delayed, and no relapse prior to vaccination. We performed sensitivity analyses to identify influential factors.
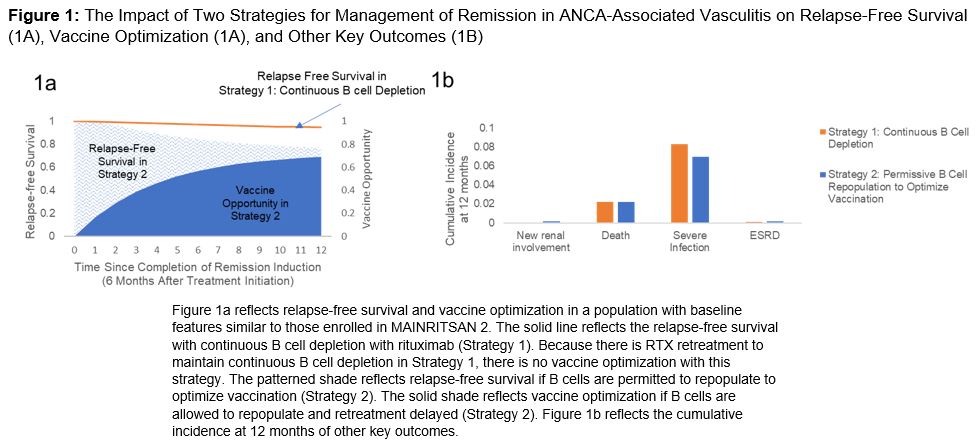
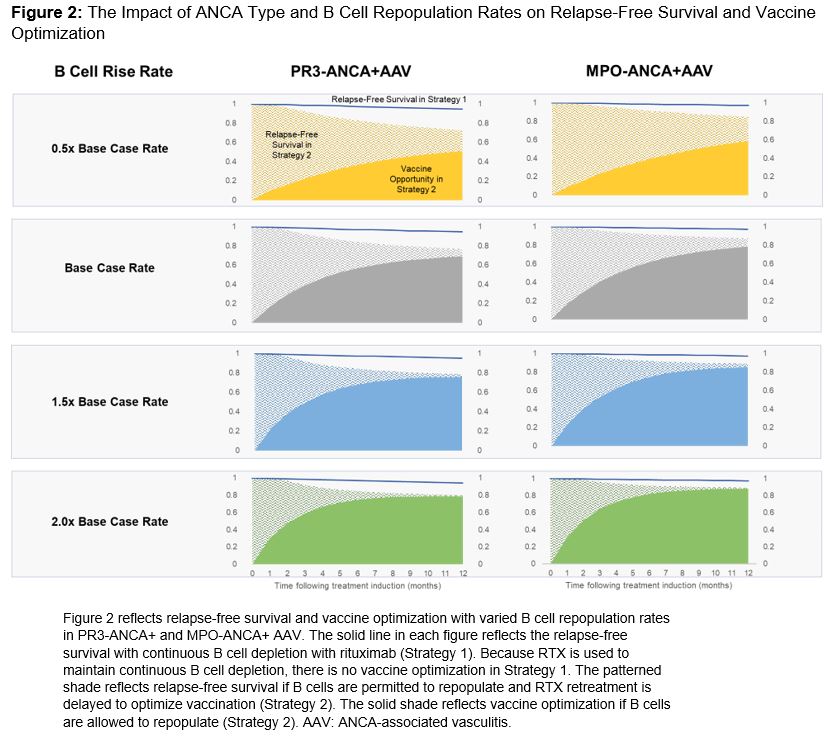
Results: Permissive B cell repopulation (Strategy 2) would be associated with lower relapse-free survival than continuous B cell depletion (Strategy 1) (81.0% vs 95.9%). However, 72.8% of patients would be optimized for vaccination in Strategy 2, whereas none would be optimized in Strategy 1 (Figure 1). Minimal differences between strategies would occur in model-projected new renal involvement, ESRD, and death. Varying B cell repopulation rates and ANCA type would strongly influence relapse-free survival. Relapse-free survival in Strategy 2 would be higher in MPO-ANCA+ vs PR3-ANCA+ across B cell repopulation rates (range, 85.0%-89.4% [difference 4.4%] vs 72.7%-80.3% [difference 7.6%], respectively) (Figure 2). Further, a greater portion of MPO- vs PR3-ANCA+ patients would have vaccine optimization across scenarios (range, 58.6%-87.9% vs 51.0%-78.5%, respectively).
Conclusion: A strategy that permits B cell repopulation would be associated with a higher risk of relapse but would optimize many patients for vaccination. ANCA type (i.e., relapse risk) and B cell repopulation rates strongly influence these risks and benefits. A strategy of permissive B cell repopulation may be more acceptable in MPO-ANCA+ AAV and people with faster B cell repopulation. B cell repopulation rates had a stronger influence on model-projected relapse-free survival in PR3- than MPO-ANCA+ AAV. To further weigh the risks and benefits of each strategy, the downstream effects of vaccination (e.g., infection severity) will be incorporated in future steps. These findings highlight the importance of improving biomarkers of relapse risk and determining predictors of B cell repopulation rate.
To cite this abstract in AMA style:
Wallace Z, Wu A, Srivatsan S, Patel N, Sparks J, Miloslavsky E, Choi H, Merkel P, Stone J, Hyle E. Projecting the Impact on Clinical Outcomes in ANCA-Associated Vasculitis of Delaying Retreatment with Rituximab for Vaccine Optimization [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/projecting-the-impact-on-clinical-outcomes-in-anca-associated-vasculitis-of-delaying-retreatment-with-rituximab-for-vaccine-optimization/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/projecting-the-impact-on-clinical-outcomes-in-anca-associated-vasculitis-of-delaying-retreatment-with-rituximab-for-vaccine-optimization/