Session Information
Date: Sunday, November 10, 2019
Title: 3S089: Health Services Research I: Clinical Perspectives (951–956)
Session Type: ACR/ARP Abstract Session
Session Time: 4:30PM-6:00PM
Background/Purpose: Knee osteoarthritis (OA) is a leading cause of chronic pain in older adults. Physical therapy (PT) decreases OA pain and consequently may reduce burden of opioid use in this population. The purpose of this study was to investigate the associations of type, dose, and timing of PT with utilization of opioids following PT in individuals with incident knee OA who had used opioids in the past or were opioid naïve, using data from a large claims database.
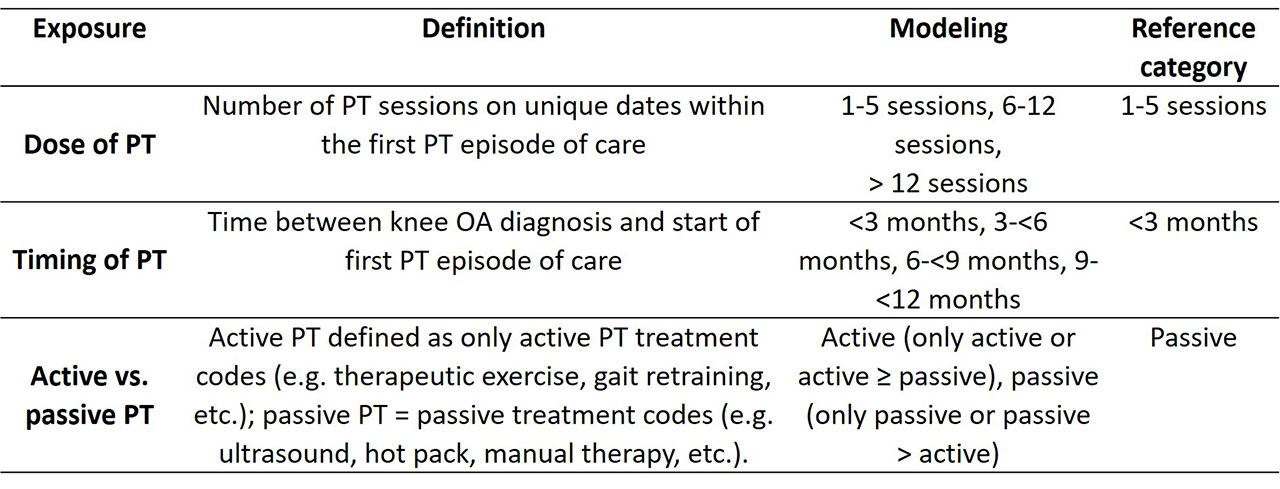
Methods: We conducted a cohort study using 2000-2014 data from the OptumLabs® Data Warehouse (OLDW), a longitudinal, real-world dataset with de-identified administrative claims and electronic health record (EHR) data. We included adults between the ages of 40-89, who after ≥ 6 months of claims data, had a knee OA diagnosis using ICD9 codes, the date of which we defined as the index date. We excluded individuals with OA-related surgeries, knee injuries, PT, cancer, or rheumatoid arthritis within 6 months prior to index date. Only persons who received PT within 12 months of the index date and who had at least 1 year of follow-up after the first PT episode of care were included. The first PT episode of care was considered to start with an initial PT evaluation followed by at least one treatment session, and was considered to end if there was a 4-week period with no PT claim or if a second evaluation was recorded. We studied several PT exposures including dose (number of sessions), timing and active versus passive modality (Table 1). The outcome was any opioid use in the 12 months after the end of the PT episode of care. Opioid use was defined as at least 2 filled prescriptions of opioids commonly used for musculoskeletal pain. Combinations of opioids with medications commonly used for cough, nasal congestion, and headache were excluded. We conducted the analyses in individuals who had used opioids prior to PT (“opioid experienced”) and those who had not used opioids prior to PT (“opioid naïve”). Covariates included age, hyperlipidemia, diabetes, and overweight/obesity. Adjusted odds (aOR) of receiving opioids were assessed (Table 1) using logistic regression.
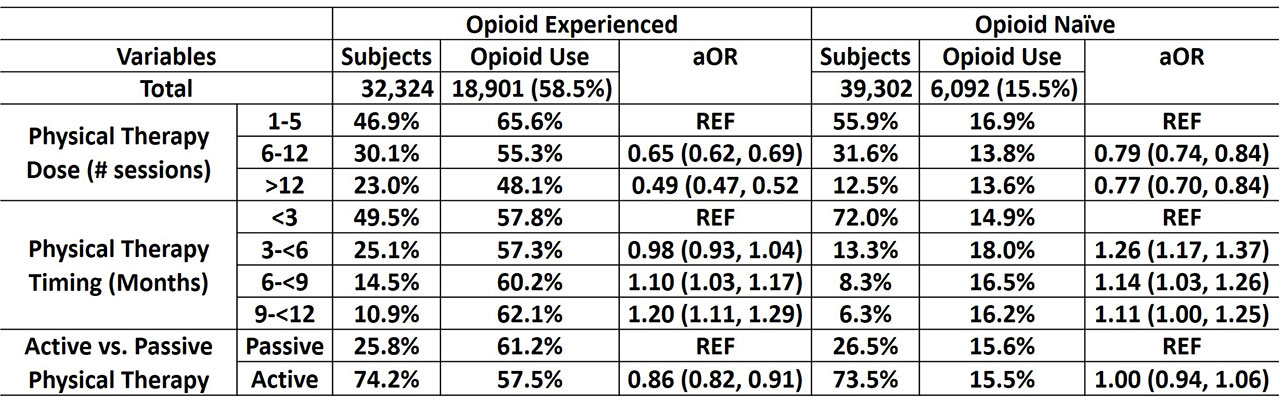
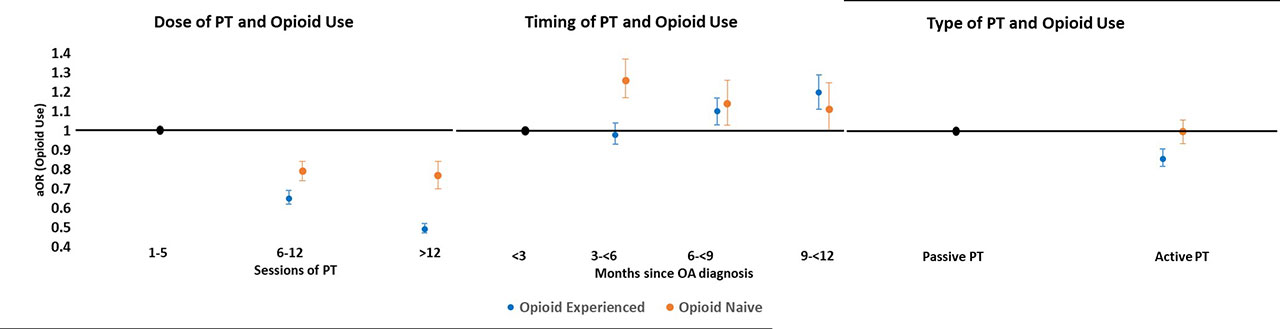
Results: We included 32,324 opioid experienced (age=60.9±10.3 years; 61.5% female) and 39,302 opioid naïve individuals (age=62.6±11.2 years; 66.0% female) (Table 2). Among both opioid experienced and opioid naïve individuals, more than 5 sessions of PT and early PT after knee OA diagnosis (vs. > 6 months) were associated with reduced odds of opioid use (Table 2, Figure 1). Among opioid naïve individuals, receiving PT >3 months after diagnosis vs. earlier was related with increase odds of opioid use (Table 2, Figure 1). Receiving active PT (vs. passive PT) was associated with reduced odds of further opioid use in opioid experienced individuals but not in the opioid naïve group (Table 2, Figure 1).
Conclusion: PT provided earlier after OA diagnosis, more than 5 sessions of PT, and use of active PT interventions may reduce opioid use in people with knee OA. These results provide guidance on optimal dosage, timing, and type of PT interventions that might be effective at reducing opioid use in this population.
To cite this abstract in AMA style:
Kumar D, Peloquin C, Stokes A, Marinko L, Camarinos J, Felson D, Dubreuil M. Physical Therapy and Opioid Use in Knee Osteoarthritis [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/physical-therapy-and-opioid-use-in-knee-osteoarthritis/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/physical-therapy-and-opioid-use-in-knee-osteoarthritis/