Session Information
Session Type: ACR Abstract Session
Session Time: 2:30PM-4:00PM
Background/Purpose: Monoclonal antibodies that inhibit nerve growth factor (NGF-abs) may offer an alternative to current nonsteroidal anti-inflammatory drug (NSAID) and opioid treatments for osteoarthritis (OA) pain and chronic low back pain (CLBP). NGF-abs differ from these treatments in several ways, including mode of administration, duration of effect, efficacy, and safety. NGF-abs also avoid some adverse effects (AEs) associated with opioids and NSAIDs—risk of physical dependence and cardiovascular risks, respectively. However, they may be associated with the risk of rapidly progressive OA (RPOA) and other AEs not seen with opioids or NSAIDs. Our objective was to quantify patients’ preferences for attributes of treatments for chronic moderate-to-severe musculoskeletal pain associated with OA and CLBP that both differentiate NGF inhibitors, NSAIDs, and opioids and are relevant to patients.
Methods: We used a discrete-choice experiment (DCE) to elicit preferences for attributes of OA and CLBP pharmaceutical treatments. The survey was completed by 602 United States residents with a self-reported physician diagnosis of hip or knee OA only, CLBP only, or comorbid OA and CLBP (OA/CLBP) diagnosed at least 3 months ago. Respondents had self-assessed moderate-to-severe pain in the hip, knee, and/or lower back, defined as a rating of 5 or greater on average in the past week on an 11-point numeric rating scale ranging from 0 (no pain) to 10 (worst possible pain). Respondents had to have taken or tried (a) 3 or more classes of pain treatment in the past 2 years, or (b) 2 prior classes of treatment if NSAIDs were contraindicated or if the patient refused to take opioids, or (c) 1 prior class of treatment if both NSAIDs were contraindicated and opioids were refused. In the DCE, respondents chose between two hypothetical treatments in a series of questions. Each hypothetical treatment was defined by six attributes: pain and symptom control, risk of RPOA, risk of heart attack, risk of physical dependence, mode and frequency of administration, and cost (Table 1). A random parameters logit model was used to estimate preferences and conditional relative attribute importance.
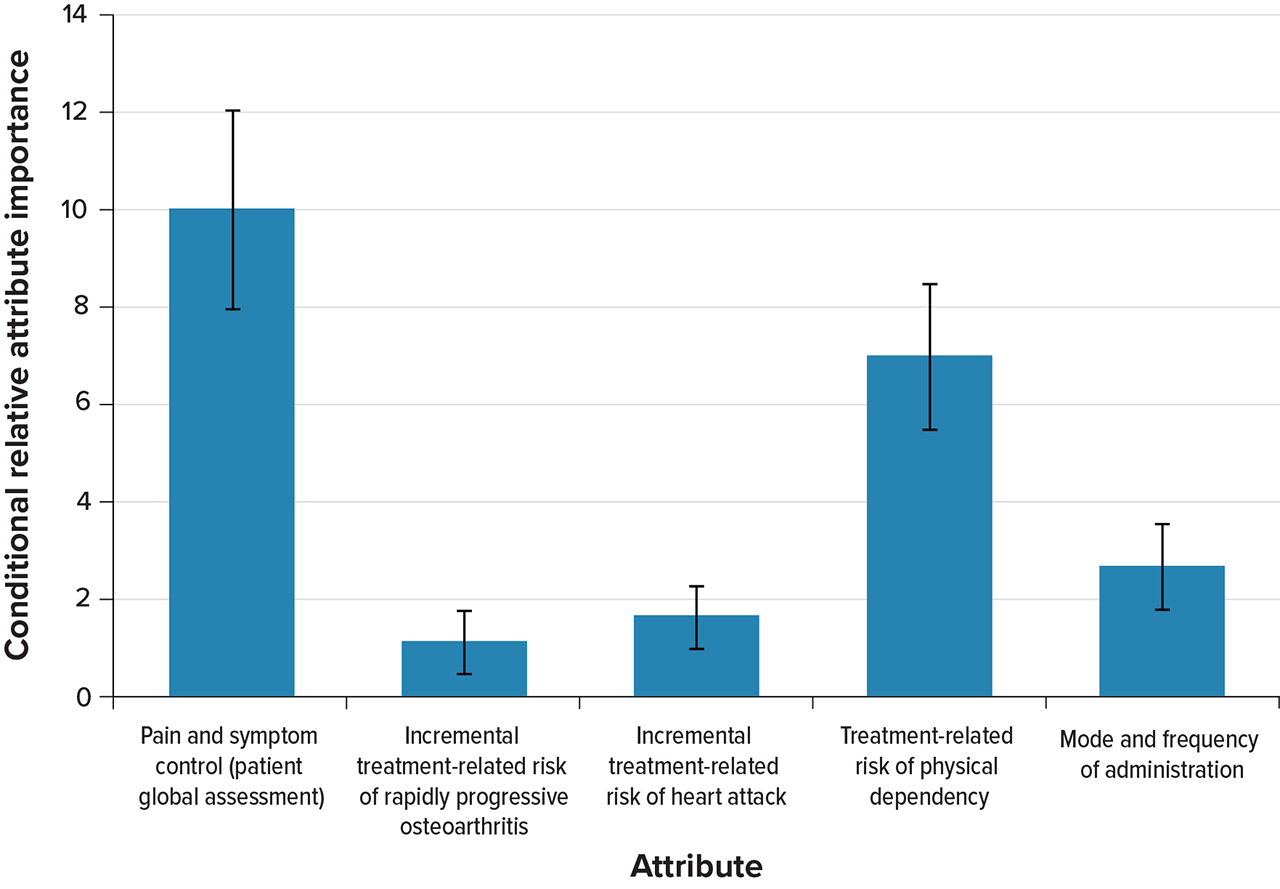
Results: Patients with OA pain only (n = 201), CLBP only (n = 202), and comorbid OA/CLBP (n = 199) completed the survey. Mean (SD) age was 63.7 (10.8) years. Mean (SD) current pain ratings for OA and CLBP were 6.4 (1.6) and 6.6 (1.4), respectively (Table 2). The relative importance of non-cost treatment attributes (mean [SE]) in descending order, rescaled so that the most important attribute was 10, was: improvement in pain and symptoms (10.00 [1.04]), risk of physical dependence (6.99 [0.74]), mode and frequency of administration (2.66 [0.43]), treatment-related risk of heart attack (1.64 [0.31]), and treatment-related risk of RPOA (1.10 [0.32]) (Figure 1).
Conclusion: Respondents were willing to accept substantial treatment-related risks to improve pain and symptoms of OA and CLBP and avoid the risk of physical dependence. Having effective alternatives to opioids is important to patients. In patients for whom NSAIDs are contraindicated, providing an effective treatment other than opioids or NSAIDs may be particularly important.

Table 1
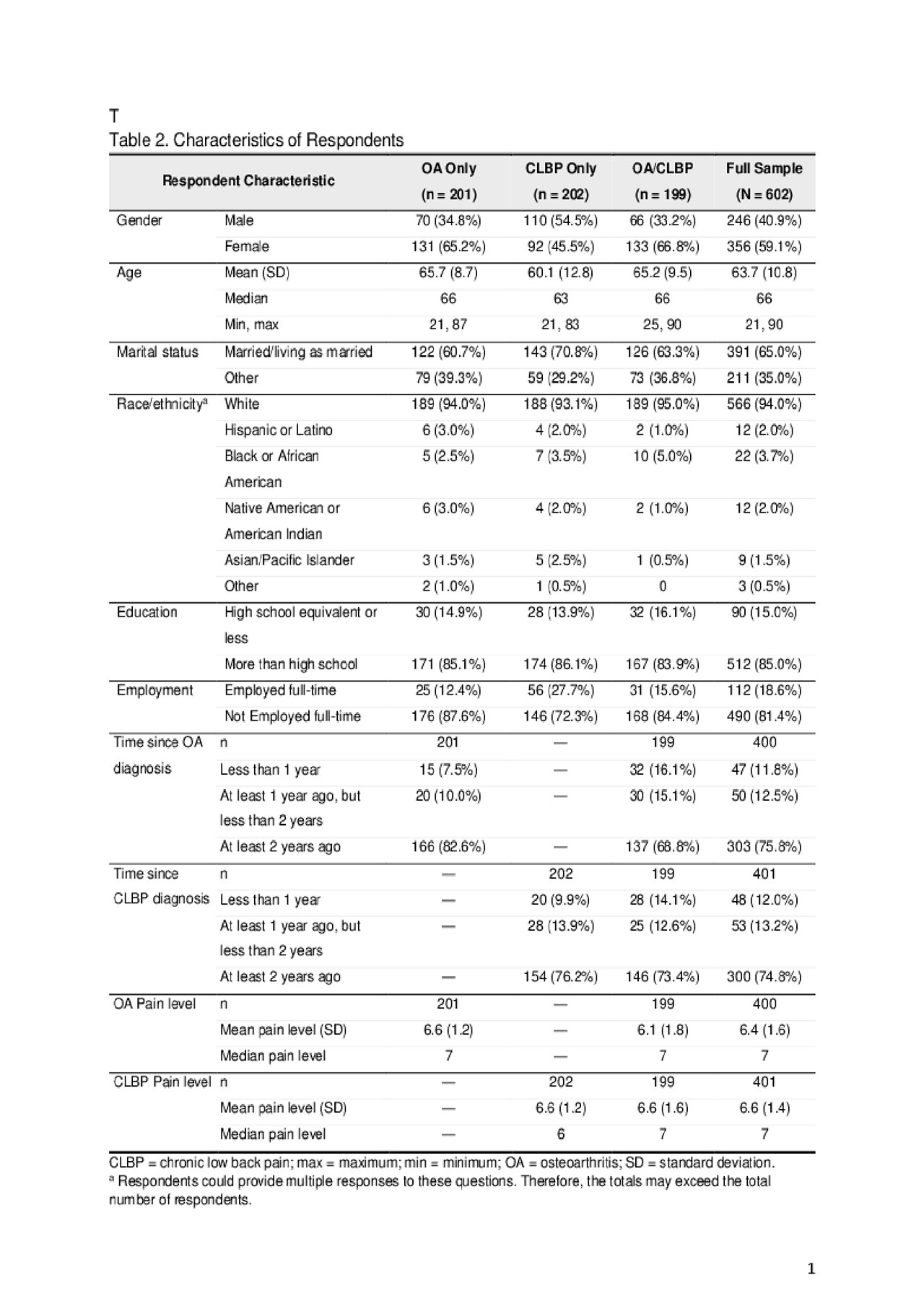
Table 2
To cite this abstract in AMA style:
Turk D, Boeri M, Abraham L, Hauber B, Atkinson J, Bushmakin A, Cappelleri J, Russo L, Viktrup L, Walsh D. Patient Preferences for Attributes of Treatments for Chronic Pain Associated with Osteoarthritis Pain and Chronic Low Back Pain That Differentiate Nerve-Growth Factor Inhibitors, Nonsteroidal Anti-inflammatory Drugs, and Opioids in the United States: A Discrete-Choice Experiment [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/patient-preferences-for-attributes-of-treatments-for-chronic-pain-associated-with-osteoarthritis-pain-and-chronic-low-back-pain-that-differentiate-nerve-growth-factor-inhibitors-nonsteroidal-anti-inf/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/patient-preferences-for-attributes-of-treatments-for-chronic-pain-associated-with-osteoarthritis-pain-and-chronic-low-back-pain-that-differentiate-nerve-growth-factor-inhibitors-nonsteroidal-anti-inf/