Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Measuring disease activity in rheumatoid arthritis
(RA) is important in evaluating efficacy of treatments, but many tests are
subjective and lead to discordance in patient and physician assessments.
Identifying factors contributing to discordance may allow disease activity to
be assessed more accurately from patient-centered assessments.
Methods: In 195 patients with RA, demographic information,
measures of disease activity, and use of therapeutic agents were assessed by
questionnaire. Patient Global Assessment (PtGA) and Physician Global Assessment
(PhGA) were assessed by marking level of disease activity on a standard 100mm
line with higher scores reflecting more disease activity (range 0-100).
Discordance in global assessment (PtGA-PhGA) was stratified into tertiles. Multiple
validated scales for an array of psychosocial comorbidities (depression,
chronic life stressors, anxiety/anger, social support, discrimination/hassles)
were assessed. Quality of life and fatigue were assessed using SF36 and FACIT
scores respectively. Multivariable (MV) linear regression was used to fit
models predicting discordance in global assessments.
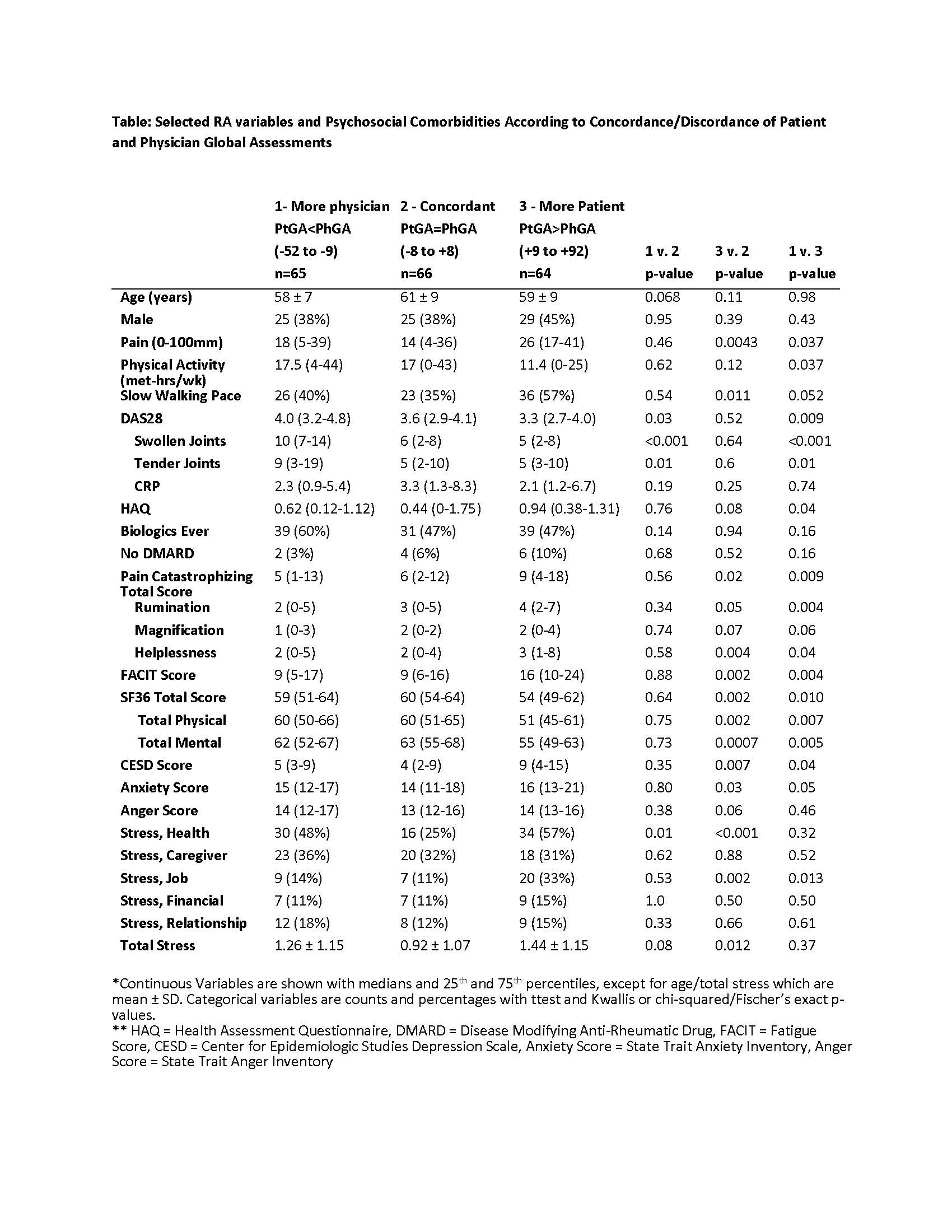
Results: Tertiles of discordance in global assessment were
defined as “Physician Higher than Patient (Ph>Pt)” [PtGA<PhGA -52 to -9
(n=65)], Concordant [PtGA=PhGA -8 to +8 (n=66)], and “Patient Higher than
Physician (Pt>Ph)” [PtGA>PhGA +9 to +92 (n=64)]. Compared with the
Pt>Ph and concordant groups, the Ph>Pt group had significantly higher
DAS28 scores with more swollen/tender joints. In contrast, the Pt>Ph group
had higher HAQ and pain/pain catastrophizing scores and was more likely to be
on no DMARDs compared with the Concordant group. Also, the Pt>Ph group had
significantly higher job stress and fatigue, depression, and anxiety scores and
lower SF36 total, physical and mental health scores along with slower walking
pace and a trend towards less physical activity. In MV models, male gender,
slower walking pace, no DMARD use, job and health stress, higher FACIT and
lower SF36 Total scores were associated with more discordance in which the PtGA
was higher than the PhGA, and more tender/swollen joints, use of a biologic and
higher anger scores were associated with more discordance in which the PhGA was
higher than the PtGA. Together, these variables explained 51% of the
discordance between patients and physicians. The psychosocial variables made up
9.4% of the explainable variability, and tender/swollen joints and slow walking
speed were the largest contributors to discordance.
Conclusion: Psychosocial comorbidities, fatigue, quality of life,
tender/swollen joints, functional status and type of therapy may explain some, but
not all, of the discordance in patient and physician assessments of disease
activity in RA.
To cite this abstract in AMA style:
Liu YL, Bathon JM, Giles JT. Multiple Psychosocial Factors Influence Subjective Assessments of Disease Activity in Rheumatoid Arthritis [abstract]. Arthritis Rheumatol. 2015; 67 (suppl 10). https://acrabstracts.org/abstract/multiple-psychosocial-factors-influence-subjective-assessments-of-disease-activity-in-rheumatoid-arthritis/. Accessed .« Back to 2015 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/multiple-psychosocial-factors-influence-subjective-assessments-of-disease-activity-in-rheumatoid-arthritis/