Session Information
Date: Tuesday, November 7, 2017
Title: Epidemiology and Public Health Poster III: Rheumatic Disease Risk and Outcomes
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Multimorbidity in Patients with Sarcoidosis: A Population-Based Cohort Study
Background/Purpose: Recent studies have suggested an increased risk of comorbidity in patients with sarcoidosis. However, whether sarcoidosis is associated with increased incidence of multimorbidity is not known.
Methods: 345 patients (50% female; 90% Caucasian, 5% African-American; mean age 45.6 years) with incident sarcoidosis in 1976-2013 in a geographically well-defined population were identified from a comprehensive medical record linkage system. Diagnosis of sarcoidosis was confirmed by individual medical record review which required diagnosis of sarcoidosis by physician supported by histopathology, compatible clinical presentation, and exclusion of other granulomatous diseases. A total of 345 sex and age-matched comparators (50% female; 95% Caucasian, 1% African-American; mean age 45.4 years) were also identified from the same underlying population. Cases and comparators were then reviewed for 18 common chronic comorbidities at index date and after index date. Aalen-Johansen methods were used to estimate the cumulative incidence of multimorbidity (defined as presence or at least 2 chronic comorbidities) adjusted for the competing risk of death. Cox proportional hazards models with adjustment for age, sex, and calendar year were used to compare the rate of development of multimorbidity between cases and comparators.
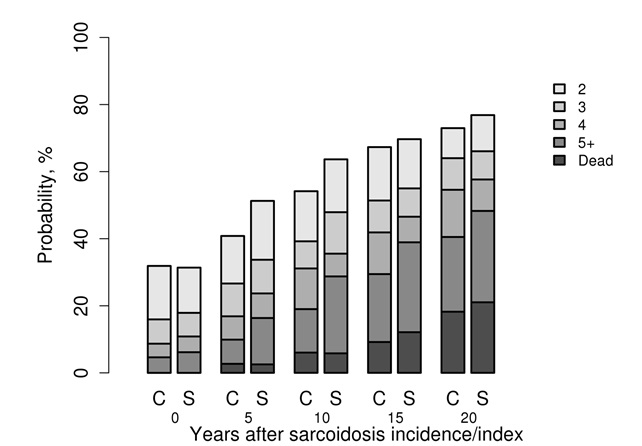
Results: At index date, 111 patients with sarcoidosis and 110 comparators without sarcoidosis had multimorbidity (p value 1.0). The mean number of comorbidities was 1.2 in both groups. During a median follow-up of 12.9 years among patients with sarcoidosis and 15.6 years among comparators, 156 patients with sarcoidosis developed multimorbidity compared to 142 comparators, corresponding to an adjusted hazard ratio of 1.60 (95% confidence interval, 1.07 – 1.69). The percentage of patients developing multimorbidity by years since sarcoidosis incidence/index date is shown in the figure. Analysis by specific comorbidity revealed significantly increased incidence of congestive heart failure, coronary artery disease, arrhythmia, cerebrovascular accident, arthritis, asthma, depression, diabetes and osteoporotic fracture after the index date among patients with sarcoidosis. The most common combination of comorbidities was hypertension and hyperlipidemia, although these were not significantly increased in sarcoidosis relative to comparators.
Conclusion: This first ever population-based evaluation of multimorbidity in sarcoidosis revealed that patients have a significantly increased incidence of multimorbidity after the diagnosis of sarcoidosis.
Figure. Probability of developing 2,3,4, 5+ comorbidities according to years since sarcoidosis incidence/ index date for patients with sarcoidosis (S) and comparators (C).
To cite this abstract in AMA style:
Ungprasert P, Matteson EL, Crowson CS. Multimorbidity in Patients with Sarcoidosis: A Population-Based Cohort Study [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/multimorbidity-in-patients-with-sarcoidosis-a-population-based-cohort-study/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/multimorbidity-in-patients-with-sarcoidosis-a-population-based-cohort-study/