Session Information
Date: Tuesday, November 12, 2019
Title: Orthopedics, Low Back Pain, & Rehabilitation Poster – ACR/ARP
Session Type: Poster Session (Tuesday)
Session Time: 9:00AM-11:00AM
Background/Purpose: The ideal treatment of swelling after TKA is unclear. The purpose of this pilot study was to determine the feasibility and initial efficacy of a multimodal edema management (MEM) program including inelastic gradient compression garment, manual lymph drainage massage and home exercise for patients presenting with swelling after TKA.
Methods: This was a prospective pilot study with retrospective historical cohort comparison. Ten patients (mean ± SD, 68 ± 2 years; 6 female) were consecutively enrolled 2 weeks prior to primary TKA. Patients were excluded if they: (1) had a chronic lower extremity swelling condition including congestive heart failure; (2) had BMI > 40; (3) had a history of thrombolytic therapy > 14 d. The multimodal therapy consisted of using an inelastic compression garment (Figure 1) 12 hours daily, self-administered manual lymph drainage massage once daily for 10 minutes, and a home exercise program (toe curling, calf pumps and knee range of motion exercises). The daily MEM program continued for 3 weeks. Primary outcomes were MEM adherence, patient satisfaction, and knee swelling quantified by bioelectrical impedance spectroscopy (BIS). Outcomes were assessed preoperatively and at 2 and 3 weeks. Secondary outcomes included quadriceps strength and activation. These outcomes were assessed preoperatively and at 3 weeks. All outcomes were re-assessed at 6 weeks. Data were compared to an historical Control group (n = 56) who met the same inclusion and exclusion criteria and who received standard physical therapy twice weekly. MEM and Control outcomes were compared using independent-samples t-tests. Preliminary effect sizes were obtained by calculating Cohen’s d statistic.
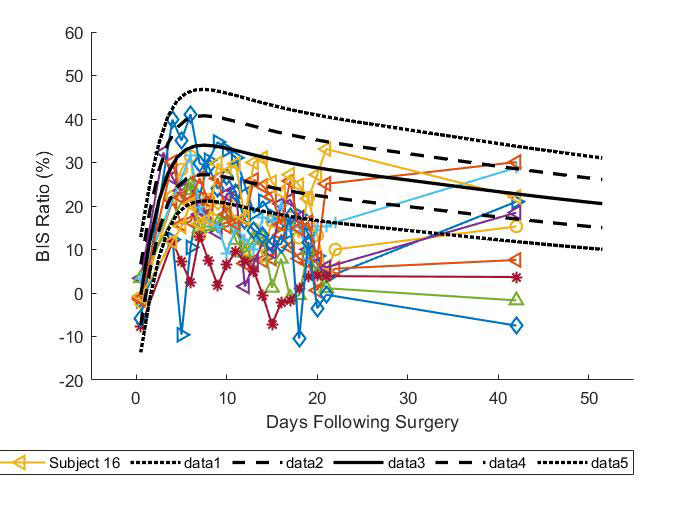
Results: Mean compression garment adherence was 81.5% for hours worn per 12-hour daily goal, and 98% for all possible days of wear. Adherence to manual lymph drainage massage and home exercise program were 100% in all patients. MEM patients were similar at baseline to Control for age, sex, body mass index, ROM, quadriceps strength and quadriceps activation (all, P >.05). Mean swelling measures for MEM were 12% lower than Control at 2 weeks (P < 0.005), and 8 of 10 patients were below the 10th percentile of Control swelling at the conclusion of the 3-week intervention period (Figure 2). At 6 weeks mean swelling reductions for MEM were 7% lower than Control (P < 0.033). Mean quadriceps activation for MEM improved 17.5% at week 6 compared to 9.4% for Control (P < 0.106) with effect sizes of 0.82 and 0.38 respectively. MEM showed smaller losses in postoperative quadriceps strength at 6 weeks compared to Control (8.2 N-m vs. 21.7 N-m; P < 0.529) with effect sizes of -0.15 and -0.40 respectively. Mean loss in active knee flexion ROM was greater for MEM than Control at 2 and 6 weeks (range 16.1 to 17.4 degrees; all, P < 0.03) but effect sizes for MEM and Control at 6 weeks for this outcome were similar at 1.11 and 1.05 respectively.
Conclusion: Use of the MEM program is feasible for treating swelling after TKA and produces improvements in swelling and quadriceps activation. Future larger randomized controlled trials are needed to determine efficacy of the MEM program and determine optimal patient characteristics for success.

To cite this abstract in AMA style:
Carmichael J, Bade M, Stevens-Lapsley J. Multimodal Edema Management After Total Knee Arthroplasty: A Pilot Study [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/multimodal-edema-management-after-total-knee-arthroplasty-a-pilot-study/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/multimodal-edema-management-after-total-knee-arthroplasty-a-pilot-study/