Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: There is strong evidence in support of increased mortality in patients with rheumatoid arthritis (RA), while the relation is more controversial in osteoarthritis (OA). Our aim was to assess mortality rates in patients with clinically relevant OA and RA, respectively, compared with those in the general population who have sought health care to minimize confounding.
Methods: We used a cohort study design within the Skåne Health Care Register in Sweden, which is a legislative, mandatory register based on physicians’ International Classification of Diseases (ICD) 10 diagnostic codes. The register covers all primary and specialist health care as well as hospitalizations in southern Sweden (population 1.3 million). The Swedish population register contains information about vital events (births, deaths) and changes in residential address. We identified all patients aged ≥45 years having received the diagnosis of knee OA (ICD-10: M17), hip OA (M16), hand OA (M18, M15.1, M15.2, M19.0D, M19.1D, M19.2D), or RA (M05, M06) during 1999 to 2006. For RA patients we required at least two health care visits with the specific code registered, with at least one from a specialist in rheumatology or internal medicine. For OA we required at least one visit with the specific code registered. For the reference population aged ≥45, we required at least one visit with any diagnostic code (90% of the population had sought care during the period). Using the population register we followed all subjects from Jan 1st 2007 until relocation outside of the region, death, or Dec 31st 2011. We calculated mortality rates using the Cox proportional hazard model adjusted for age and sex, disposable income, marital status, and highest level of education reached (provided by Statistics Sweden). In a sensitivity analysis, we considered subjects who received a diagnosis of pain in a joint (M25.5, location unspecified) at age 55 or older as OA subjects in addition to the definition above.
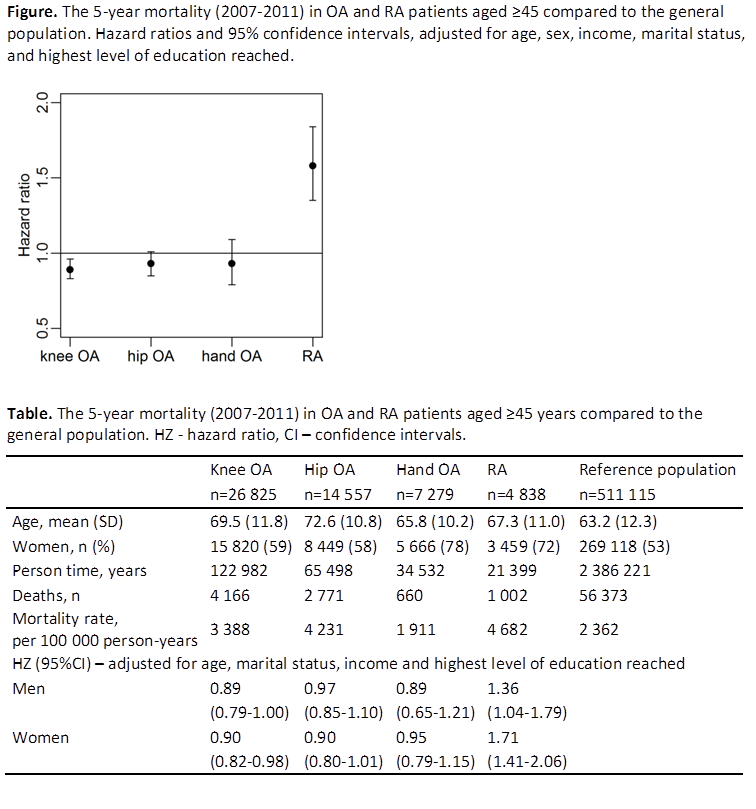
Results: The hazard ratio of death for RA patients compared to general population was 1.58 (95% CI: 1.35-1.84). Patients with knee, hip or hand OA did not have increased risk of mortality compared with the general population, adjusted for age, sex and socioeconomic variables (Figure). The risk of death remained similar when OA in any joint (i.e., any combination of knee, hip, or hand) was assessed, or when pain in a joint at age ≥55 was additionally considered as OA. Effect estimates were similar in men and women (Table).
Conclusion: We found no evidence of increased risk of mortality over 5 years in patients with doctor-diagnosed knee, hip or hand OA, compared with the general population, while increased mortality in RA was confirmed.
Disclosure:
A. Turkiewicz,
None;
T. Neogi,
None;
G. Peat,
None;
M. Englund,
None.
« Back to 2013 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/mortality-in-clinically-relevant-osteoarthritis-and-rheumatoid-arthritis-compared-with-the-general-population/