Session Information
Date: Sunday, October 26, 2025
Title: (0233–0279) Miscellaneous Rheumatic & Inflammatory Diseases Poster I
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Monogenic autoinflammatory diseases are rare innate immunity disorders characterized by recurrent episodes of fever and systemic inflammation. They are most often described in childhood, although adult-onset cases have been reported. Clinical, genetic, and phenotypic expression varies by geographic region, and correlations between genotype and symptomatology have been described.Undefined autoinflammatory syndrome (uSAID) is characterized by recurrent episodes of inflammation similar to monogenic autoinflammatory diseases with no diagnosis or genetic alterations detected.The purpose of this study is to describe the characteristics of autoinflammatory diseases managed in rheumatology and to analyze genotype–phenotype correlations in patients with Familial Mediterranean Fever (FMF).
Methods: Descriptive, longitudinal, retrospective study of patients with monogenic autoinflammatory diseases and uSAID in the Rheumatology Department of a tertiary hospital. Demographic, diagnostic and clinical data were registered throughout the disease course. Laboratory, Autoinflammatory Disease Activity Index (AIDAI) and therapeutic data at the last visit were collected. Student’s T-test and Pearson correlation matrix were applied for analytical modeling.
Results: 70 patients were studied (60% female), with a median age at symptom onset of 10.3 years (±14.9) and at diagnosis of 18.4 years (±15.3). Table 1 describes their demographic, clinical and laboratory features.A positive correlation was observed between amyloid levels and ESR, and more strongly with CRP. Higher levels of amyloid, CRP, and ESR were associated with older age at symptom onset, diagnosis, and beginning of follow-up. Female sex was linked to higher ESR levels and later diagnosis (median in males 13 vs. 31 years in females). Additionally, higher AIDAI scores were associated with requirement for anti-IL1 therapy.Among FMF patients, 15 (41%) were compound heterozygotes (symptom onset at 5.6 years [SD 6.8]), 17 (47%) simple heterozygotes (symptom onset 12.8 years [SD 16]), and 3 (8%) homozygotes (symptom onset 13 years [SD 14.5]). Table 2 shows FMF patient characteristics according to genotype. Symptom onset was statistically significantly earlier in compound than in simple heterozygotes (p = 0.0137; see Figure 1).18 MEFV gene mutations were identified in FMF patients. The most frequent were c.2082G >A (p.Met694Ile) (25%), c.442G >C (p.Glu148Gln) (19%), and c.2080A >G (p.Met694Val) (16%). Among patients with uSAID, 22% were in remission without treatment, 11% received colchicine, and 61% required biologic therapy.
Conclusion: -Amyloid levels were correlated with the need for anti-IL1 therapy; female sex was associated with later diagnosis and higher ESR levels. -FMF was the most frequent disease, being c.2082G >A (p.Met694Ile) the most common MEFV mutation observed. -FMF patients with compound heterozygosity showed more typical clinical features with a higher proportion of patients meeting classification criteria, and symptom onset was statistically significantly earlier than in simple heterozygotes. -Most patients uSAID did not respond to colchicine and required biologic therapy, mainly anakinra.
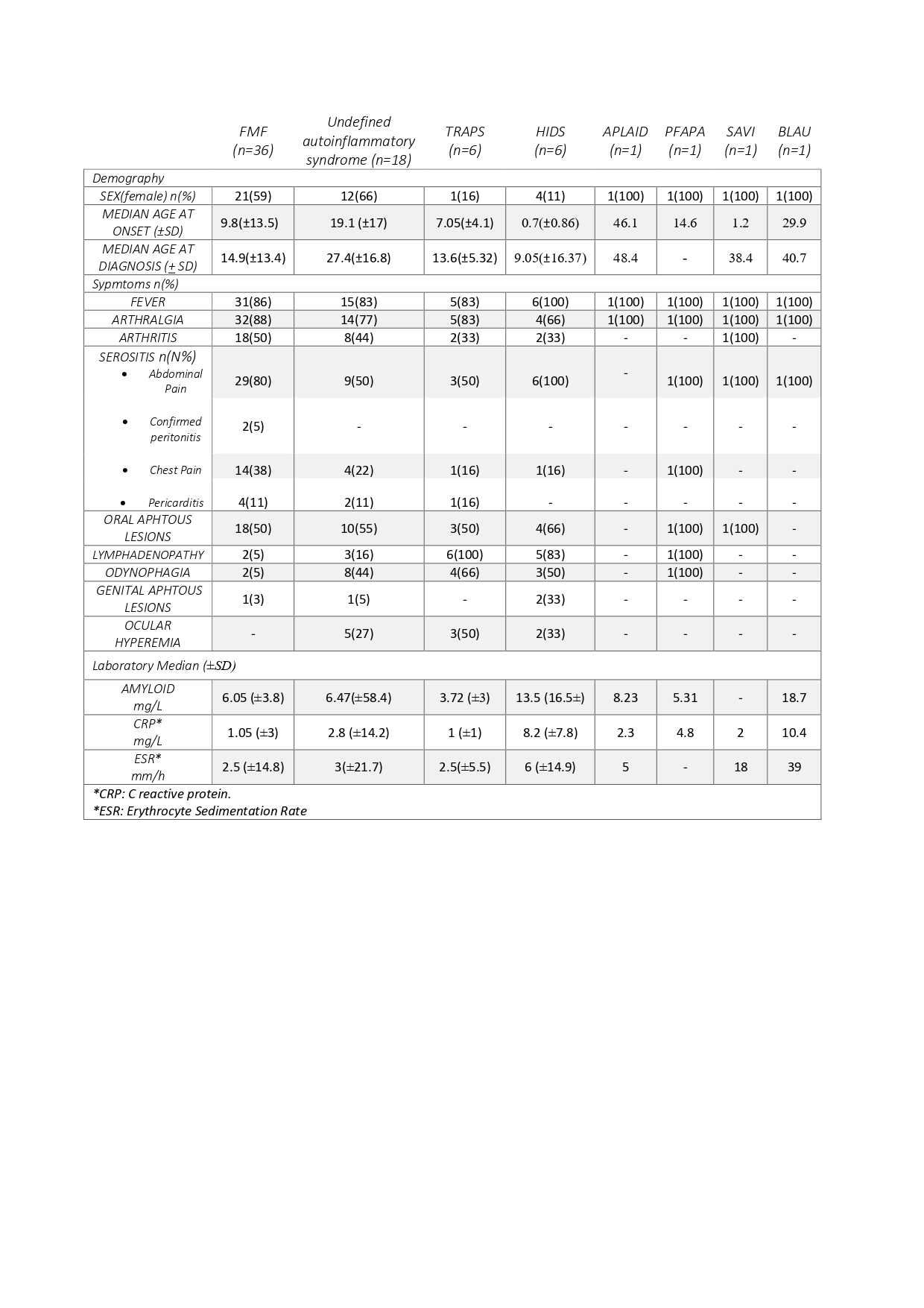 Table 1. Demographic, clinical and laboratory features of the patients studied by diagnosis.
Table 1. Demographic, clinical and laboratory features of the patients studied by diagnosis.
.jpg) Figure 1. Distribution of symptom onset age according to FMF patient genotype.
Figure 1. Distribution of symptom onset age according to FMF patient genotype.
.jpg) Table 2. Classification criteria and treatment according to FMF patient genotype.
Table 2. Classification criteria and treatment according to FMF patient genotype.
To cite this abstract in AMA style:
Torrat Noves A, Ivorra Cortes J, Mateo Vendrell A, GRAU GARCIA E, Muñoz Martinez P, Mas Sanchez L, Ramos Castro D, Alcántara Álvarez I, Villanueva Manes B, perez Hurtado A, Simeo Vinaixa M, Calvo Penades i, López Montesinos B, Lacruz-perez L, Andrés Román Ivorra J. Monogenic autoinflammatory diseases and undefined autoinflammatory syndrome in Western Mediterranean adults: clinical, genetic, and therapeutic insights [abstract]. Arthritis Rheumatol. 2025; 77 (suppl 9). https://acrabstracts.org/abstract/monogenic-autoinflammatory-diseases-and-undefined-autoinflammatory-syndrome-in-western-mediterranean-adults-clinical-genetic-and-therapeutic-insights/. Accessed .« Back to ACR Convergence 2025
ACR Meeting Abstracts - https://acrabstracts.org/abstract/monogenic-autoinflammatory-diseases-and-undefined-autoinflammatory-syndrome-in-western-mediterranean-adults-clinical-genetic-and-therapeutic-insights/