Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: Impact of dermatological disease is measured with the Dermatology Life Quality Index (DLQI) and Skindex-17. DLQI is commonly used in dermatology trials but the Skindex-17 has better psychometric properties and less floor effect. We aim to describe health-related quality of life (HRQoL) related to skin involvement using the DLQI and Skindex-17 and to assess impact of replacing DLQI by the Skindex-17 in determining overall PsA disease activity.
Methods: Data collected in the ongoing Dutch south-west Early Psoriatic Arthritis CohoRt (DEPAR) and used for this analysis were Psoriasis Area and Severity Index (PASI) , DLQI (range 0-30) and the Skindex-17 (Domains: Psychosocial 0-24 and Symptoms 0-10). Spearman’s correlation was used to calculate correlation between questionnaires and correlation between change in questionnaire-score and change in PASI. The latter was performed within subgroups of psoriasis severity (PASI<7, 7-12 and >12) using change in the first three months after baseline. In the Composite Psoriatic Disease Activity Index (CPDAI), skin involvement is considered not involved, mild, moderate or severe. Using cutoff values of Skindex-17 Symptoms >5 and/or Skindex-17 Psychosocial >9, reclassification of skin assessment was analyzed.
Results: In total 1657 questionnaires of 390 patients were available (mean age 50 years, 51% male). At baseline, median DLQI was 1 (interquartile range, IQR 0-5), Skindex-17 Symptoms 4 (IQR 2-6) and Skindex-17 Psychosocial 2 (IQR 0-8). Correlation between DLQI and Skindex-17 domains was 0.78 (p<0.05). In mild psoriasis (PASI 0-7, n=200), change in PASI had a significant but low correlation with change in HRQoL (Table 1). In moderate psoriasis (PASI 7-12, n=27) the correlation was higher. 269 cases (16%) had CPDAI reclassification, the majority changing from mild with DLQI to moderate with Skindex-17 (n=250, Table 2).
Conclusion: In early PsA with mild/moderate psoriasis, impact of psoriasis is best reflected in the Skindex-17. Using the Skindex-17 in the CPDAI leads to higher rating of skin involvement than using the DLQI. Both suggest a more subtle impact on HRQoL is missed in the DLQI and the Skindex-17 is preferred in PsA. 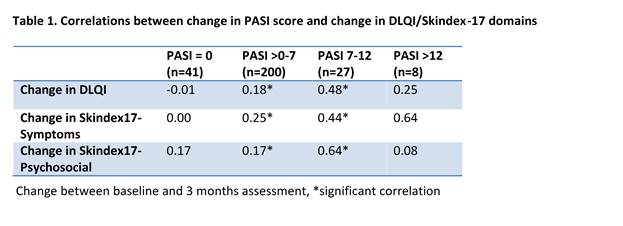

To cite this abstract in AMA style:
Wervers K, Luime JJ, Tchetverikov I, Gerards AH, Kok MR, Appels CWY, van der Graaff WL, van Groenendael JHLM, Korswagen LA, Veris J, Hazes JMW, Vis M. Measuring Psoriasis Specific Impact on Quality of Life: Performance of Dlqi and Skindex-17 in Early Psoriatic Arthritis [abstract]. Arthritis Rheumatol. 2017; 69 (suppl 10). https://acrabstracts.org/abstract/measuring-psoriasis-specific-impact-on-quality-of-life-performance-of-dlqi-and-skindex-17-in-early-psoriatic-arthritis/. Accessed .« Back to 2017 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/measuring-psoriasis-specific-impact-on-quality-of-life-performance-of-dlqi-and-skindex-17-in-early-psoriatic-arthritis/