Session Information
Session Type: Poster Session A
Session Time: 10:30AM-12:30PM
Background/Purpose: Hand manifestations (limited joint mobility, [LJM]; flexor tenosynovitis, [FT]; carpal tunnel syndrome, [CTS]; Dupuytren disease, [DD]) are common complications in diabetes. Despite their heterogeneity in presentation, all manifestations share a common pathophysiologic process of pro-fibrotic inflammation in flexor structures. Unifying measures of disease severity across these conditions are lacking. We studied prevalence and severity in diabetes, prediabetes and controls, and assessed the utility of measuring mean metacarpophalangeal joint (MCP) extension in these conditions.
Methods: We studied 2405 adult individuals with Type 1 diabetes (n=291), Type 2 diabetes (n=877), prediabetes (n=326) and non-diabetic controls (n=911). Comprehensive clinical evaluations assessed hand symptoms, signs (Tinel sign, tenosynovial thickening), function (hand grip strength, Duruoz Hand Index, [DHI]). Mean MCP extension was calculated as an average of maximum passive extension of 2nd-5th finger of each hand, measured by a protractor. A rheumatologist or diabetes specialist opined independently on the manifestation present; skin thickening (ST) was classified when there was no prayer sign. Data on diabetes duration, medications, complications were collected. We compared mean MCP extension in diabetes versus controls (ANOVA adjusted for age and sex) and in those with hand manifestations versus those without.
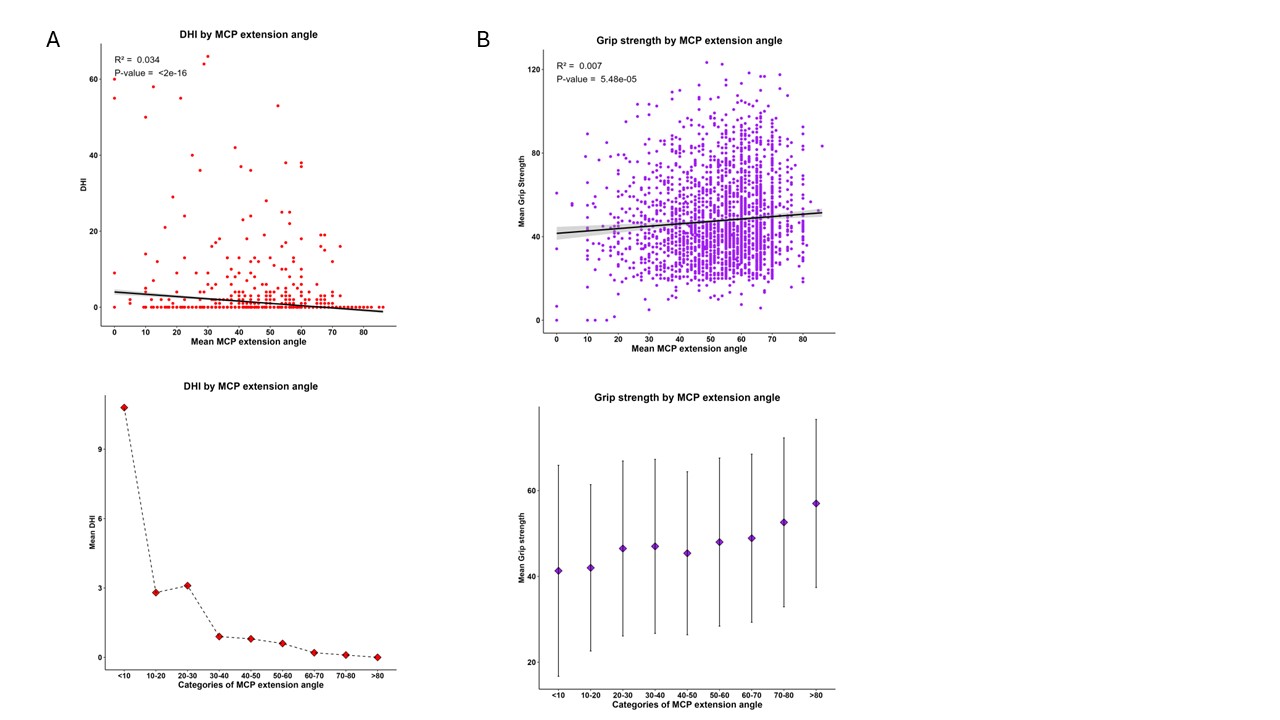
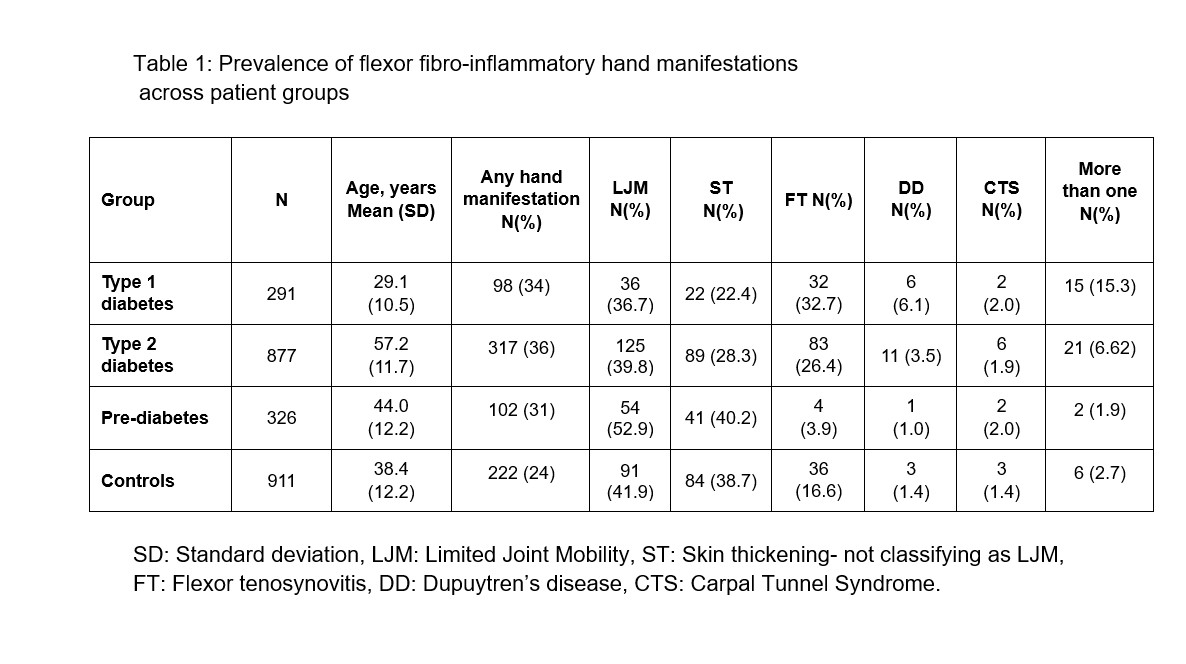
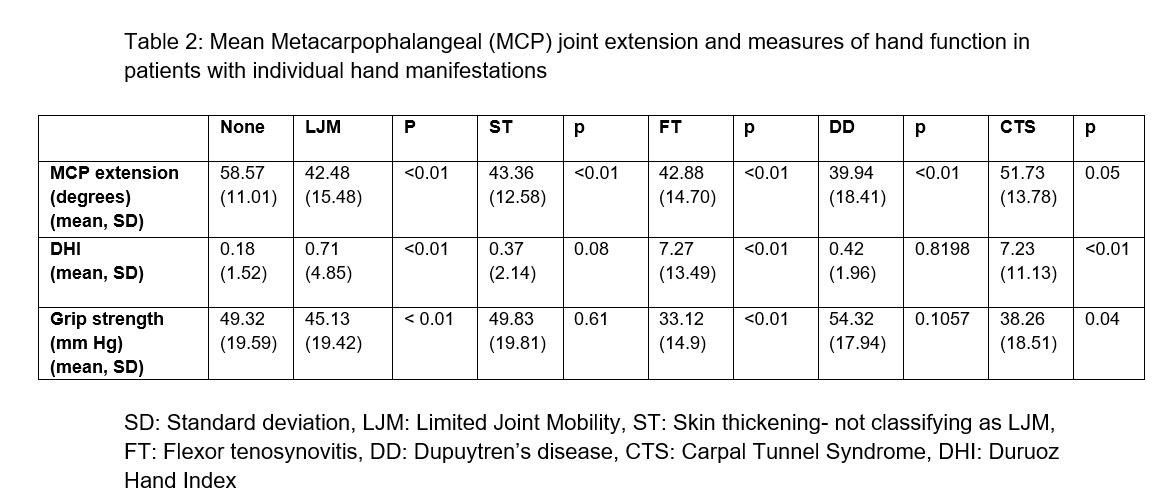
Results: Approximately one third patients with diabetes (34% Type 1, 36% Type 2) and prediabetes (31%) had hand involvement, as compared to 24% in controls (Table 1). As a group, mean MCP extension was lower in Type 2, Type 1 and prediabetes when compared with controls (all p< 0.01). Across all groups, Mean MCP extension was hampered in patients with LJM, ST, FT and DD (all p< 0.01 compared to those with no hand manifestations) but not in CTS. (p=0.053) (Table 2). Grip strength was significantly lower only in LJM and CTS but not in the others manifestations. MCP extension angle correlated with DHI (R = 0.17, p< 0.01, Figure 1A) and grip strength (R = 0.26, p< 0.01, Figure 1B); DHI was elevated mainly in those with MCP extension < 30 degrees. (Figure 1). A regression model in the diabetic population (Type 1 and Type 2) showed that Mean MCP angle was associated with diabetes duration (p< 0.01) and microvascular complications (p=0.03) but not insulin use, body mass index (BMI), macrovascular complications, history of frozen shoulder or liver disease.
Conclusion: Our findings underscore the high prevalence of flexor hand manifestations, often asymptomatic, in diabetes and controls. MCP extension is a potential marker of the extent of hand fibrosis in LJM, FT and DD, picking up early involvement without functional limitation. This simple and non-invasive technique offers a quantitative measure of hand involvement that will allow correlations with markers of fibrosis in other organs and as an outcome measure for responses to medical and surgical treatments in these conditions.
To cite this abstract in AMA style:
Phatak S, Wagh R, Dhadge S, Jadhav S, Ladha P, Nalkande R, Shah R, Ingram J, Yajnik C. Mean Metacarpophalangeal Extension to Clinically Quantify Flexor Fibro-inflammatory Hand Involvement in Diabetes [abstract]. Arthritis Rheumatol. 2024; 76 (suppl 9). https://acrabstracts.org/abstract/mean-metacarpophalangeal-extension-to-clinically-quantify-flexor-fibro-inflammatory-hand-involvement-in-diabetes/. Accessed .« Back to ACR Convergence 2024
ACR Meeting Abstracts - https://acrabstracts.org/abstract/mean-metacarpophalangeal-extension-to-clinically-quantify-flexor-fibro-inflammatory-hand-involvement-in-diabetes/