Session Information
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: Lupus low disease activity state (LLDAS) (Ann Rheum Dis. 2016;75:1615–21.) combine both low disease activity (SLEDAI score of ≤4, PGA >=1 no flare, no severe organ involvement) and prednisone reduction ( >= 7.5 mg). Being in LLDAS for 50% or more of follow-up visits results in a 50% reduction in organ damage (Arthritis Rheumatol 2018;70:1790-5). LLDAS has been a useful secondary outcome measure in randomized clinical trials. We asked whether being in LLDAS at the start of pregnancy predicted the pregnancy outcome.
Methods: All patients met revised ACR or SLICC classification criteria. At each visit, LLDAS was calculated. The start date of each pregnancy was determined. At each visit, we created a variable to indicate the trimester of the pregnancy. To evaluate whether LLDAS at the first pregnancy visit associated with pregnancy outcomes, a GEE model was used to account for the same patient contributing more than one pregnancy.
Results: There were 636 pregnancies (from 435 patients: 36% African American, 54.5% Caucasian) that had LLDAS status determined at the first pregnant visit. Of these 636 pregnancies, there were 537 births, 77 miscarriages, and 22 terminations. 291 patients had 1 pregnancy, 100 had 2, and 44 had 3 recorded. There was no association between reaching LLDAS at the first pregnancy visit and miscarriage (OR 0.71, 95% CI 0.44, 1.15, p=0.16, adjusted for age and race). Table 1 shows the association between LLDAS at the first pregnancy visit and preterm birth, with 537 pregnancies eligible for analysis. There was strong evidence of an association between LLDAS at first pregnant visit and preterm birth. Next, we looked at pregnancies that had the first visit in the first trimester. There were 462 pregnancies included. Once again, there was no association with miscarriage (OR 0.76, 95% CI 0.45, 1.29 p=0.312 adjusted for age and race). Table 2 shows the analysis of being in LLDAS at the first trimester and preterm birth (396 pregnancies were eligible for analysis). The same strong protective effect of being in LLDAS against preterm birth was found.
Conclusion: Currently, women with SLE are told that their SLE should be “in remission” for 6 months prior to conception. Our data suggest that being in LLDAS may be sufficient to protect against preterm birth, which numerically remains the most frequent adverse pregnancy outcome in SLE. LLDAS does not protect against miscarriage (likely because antiphospholipid antibodies contribute to miscarriage risk). LLDAS is a more realistic pre-pregnancy clinical goal, as durable remission is difficult to achieve in SLE.
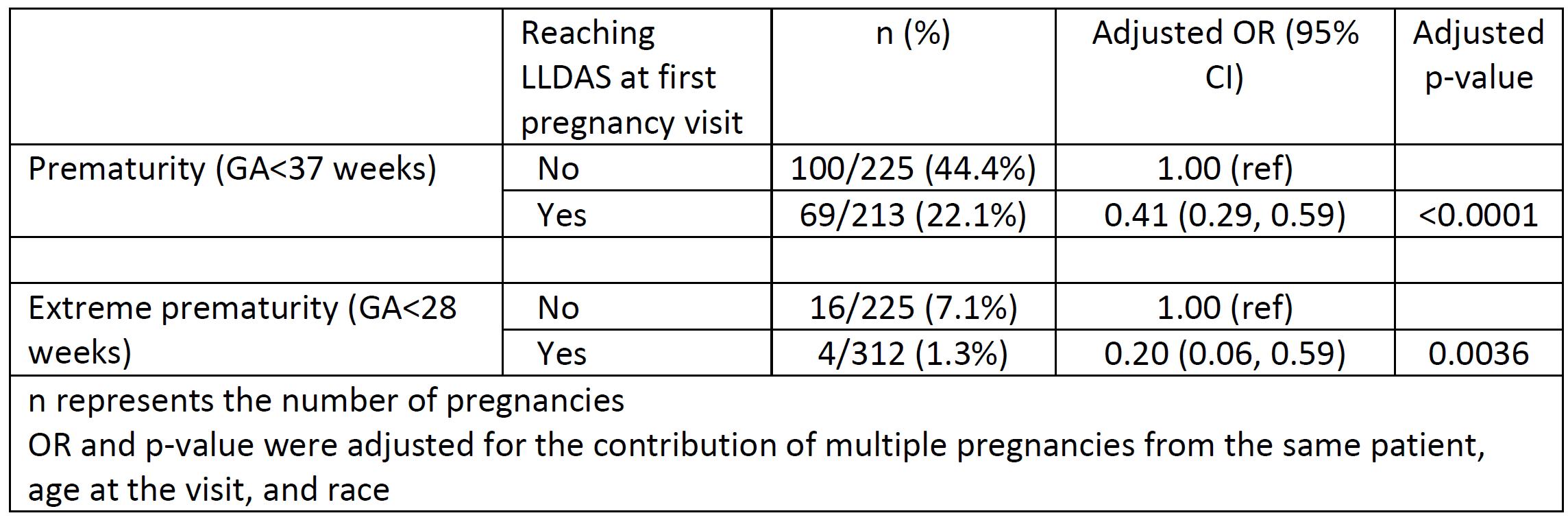 Table 1: Association between LLDAS at first pregnancy visit and preterm birth
Table 1: Association between LLDAS at first pregnancy visit and preterm birth
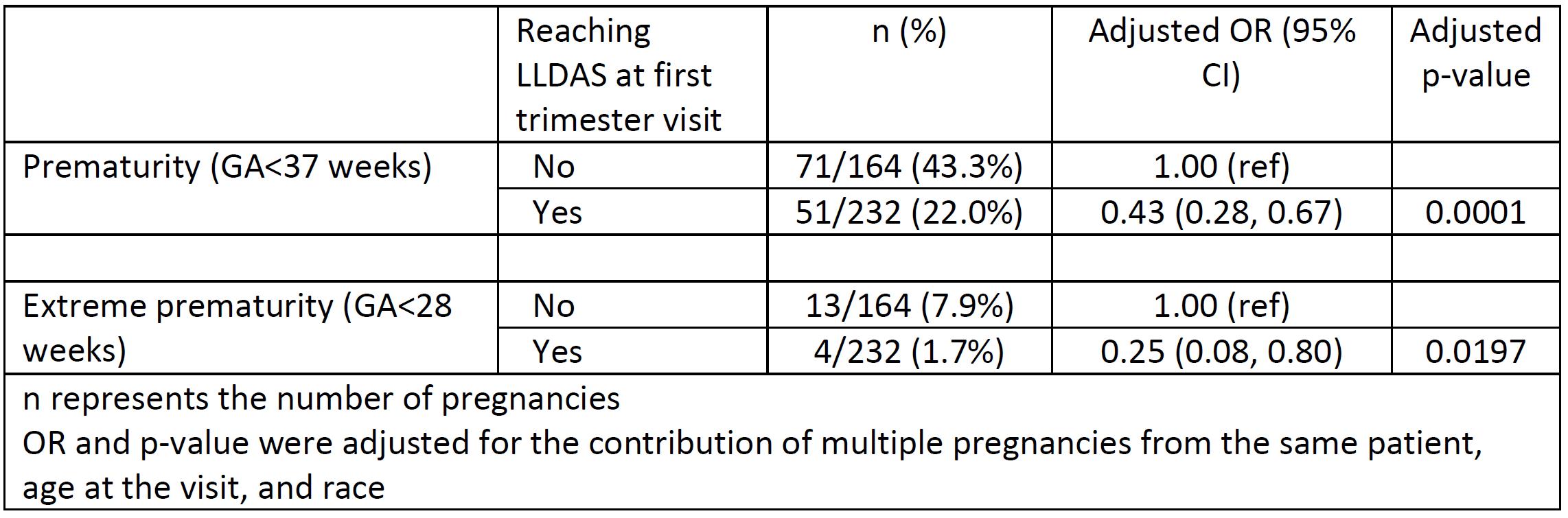 Table 2: Association between LLDAS at first trimester visit and preterm birth
Table 2: Association between LLDAS at first trimester visit and preterm birth
To cite this abstract in AMA style:
Petri M, Li J, Goldman D. Lupus Low Disease Activity State Protects Against Pre-Term Birth [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/lupus-low-disease-activity-state-protects-against-pre-term-birth/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/lupus-low-disease-activity-state-protects-against-pre-term-birth/