Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: interstitial lung disease (RA-ILD) is one of the most serious extraarticular complications of rheumatoid arthritis (RA). Presently, it is not clear which is the best strategy for the detection of RA-ILD. We have previously reported on the feasibility and accuracy of lung ultrasound (LUS) in the detection of RA-ILD (1). Aim of the present study was to assess the performance of LUS in the detection of RA-ILD in clinical practice, and to compare its accuracy with the detection algorithms usually adopted.
Methods: 147 unselected RA patients (114 F and 33 M) were studied. In all patients, LUS was performed as previously described (1) by an expert physician (MC), blinded to clinical and HRCT data, using a standard commercially available US equipment (Esaote MyLabFive) with a 7.5-12 MHz probe. By LUS, RA-ILD was defined by a B-lines score >10. The results of the LUS study were compared to clinical, pulmonary function tests, chest X-ray, and lung CT (HRCT) data, as available from clinical records. Four clinical algorithms (ALG) were identified: ALG 1: presence of dyspnea (NYHA class >=2) and/or bibasilar crackles; ALG 2: as ALG 1 + FVC < 80%; ALG 3 as ALG 1 + DLCO<80%; ALG 4 as ALG 1 + evidence of ILD at chest X-ray. Sensitivity, specificity, and predictive values of LUS and clinical algorithms with reference to HRCT were calculated, and compared by McNemar test.
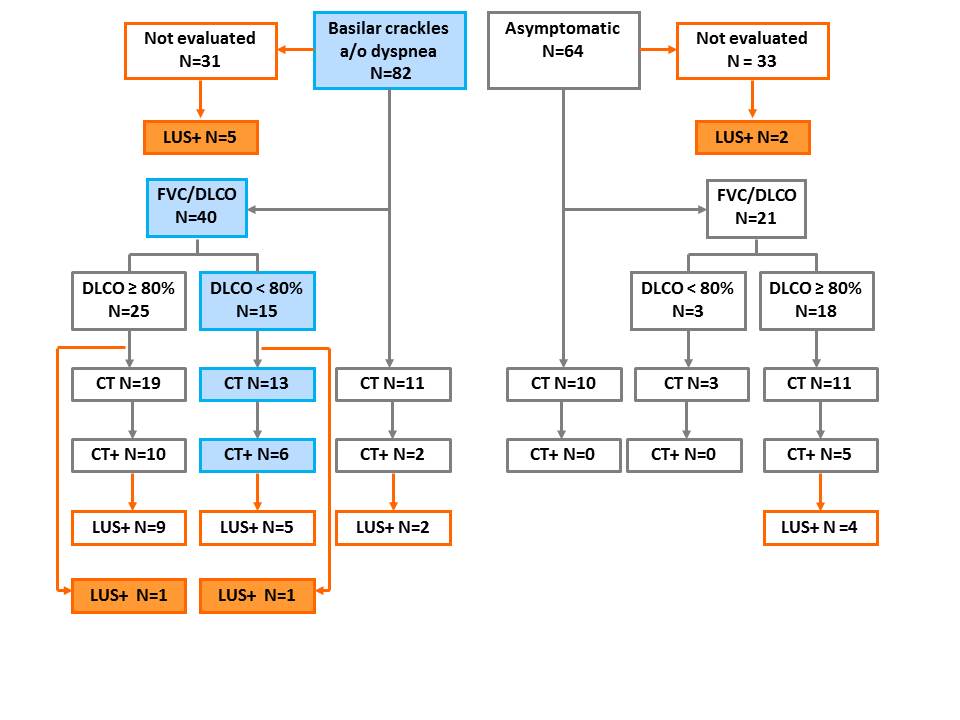
Results: RA-ILD was detected by LUS in 41/146 (28.1%) patients. Clinical data, FVC, DLCO, X-ray, and CT were available in 146(100%), 63(43%), 61(42%), 102(70%), and 67(46%) cases respectively. LUS showed a significantly higher accuracy in the detection of RA-ILD than clinical algorithms (Table 1). 33/64(52%) asymptomatic patients, and 31/82(38%) patients with clinical suspicion of RA-ILD, were not further evaluated by neither PFTs nor by HRCT. Overall, LUS detected unsuspected signs of RA-ILD in 9/146(6%) patients (Fig 1).
Conclusion: LUS is more accurate than usual clinical algorithms in the evaluation of RA-ILD, and allows the detection of a substantial number of unsuspected cases.
Tab. 1 – Sensitivity, specificity, and predictive power of LUS and clinical algorithms in the detection of RA-ILD. HRCT is the gold standard.
|
||||||
|
LUS
|
ALG 1 (crackles a/o dyspnea)
|
ALG 2 (ALG 1 + FVC < 80%) |
ALG 3 (ALG 1 + DLCO < 80%) |
ALG 4 (ALG 1 + X-ray +)
|
||
|
|
|
|
|
|
||
|
Sensitivity % (IC 95%)
|
87.0 (76.0 – 93.6) |
78.3 (66.2 – 87.0)
|
9.5 (3.3 – 22.7) |
47.6 (32.9 – 62.7) |
41.7 (26.7 – 58.2) |
|
|
Specificity, % (IC 95%)
|
72.7 (60.3 – 82.6) |
43.2 (31.3 – 55.8) |
96.0 (84.4 – 99.4) |
52.0 (37.0 – 66.7) |
89.3 (74.5 – 96.3) |
|
|
PPV % (IC 95%)
|
62.5 (49.8 – 73.8) |
41.9 (30.1 – 4.5)
|
66.7 (51.1 – 79.4) |
45.5 (31.0 – 60.7) |
62.5 (45.8 – 76.8) |
|
|
PPN% (IC 95%)
|
91.4 (81.4 – 96.5) |
79.2 (67.2 – 87.8) |
55.8 (40.5 -70.1) |
54.2 (39.0 – 68.7) |
78.1 (61.8– 89.1) |
|
|
p * |
total |
–
|
0.02 |
0.005 |
0.05 |
0.05 |
|
sensitivity |
– |
0.687 |
0.000 |
0.021 |
0.070 |
|
|
specificity |
– |
0.007 |
0.039 |
0.549 |
0.227 |
|
|
McNemar test: * = p refers to the comparison of LUS with clinical algorithms |
||||||
Fig 1: LUS RA-ILD in the population (LUS+). Orange-filled boxes show LUS-positive patients which were unsuspected on clinical ground
References: Cogliati C, et al. Rheumatology (Oxford). 2014 Mar 31. [Epub ahead of print]
Disclosure:
M. Antivalle,
None;
M. Chevallard,
None;
M. Battellino,
None;
M. Ditto,
None;
V. Varisco,
None;
F. Rigamonti,
None;
A. Mutti,
None;
F. Atzeni,
None;
A. Batticciotto,
None;
P. Sarzi-Puttini,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/lung-ultrasound-screening-for-interstitial-lung-disease-in-rheumatoid-arthritis-comparison-with-usual-detection-algorithms-in-clinical-practice/