Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Interstitial lung disease (ILD) is a feared complication of several pediatric rheumatic diseases, particularly dermatomyositis. Lung transplant is often considered as a last resort in these patients, which can lead to delayed transplant assessment and listing in a population for which suitable organs are already difficult to procure, ultimately resulting in high mortality. Furthermore, certain myositis-specific and myositis-associated antibodies, such as antibodies to melanoma differentiation-associated protein 5 (MDA5- ab) and those implicated in anti-synthetase syndrome, are associated with a rapidly progressive ILD phenotype which requires early recognition and expedited referral to lung transplant centers to reduce morbidity/mortality.
Methods: We present a case series of three patients with ILD due to dermatomyositis, two with anti-MDA5-ab positivity, and a third with anti-PM/Scl100 who had features of an anti-synthetase-like syndrome. Laboratory, imaging and pathology features unique to each case are presented, along with the clinical course and outcome of each patient.
Results: All three patients were female, with ages at disease onset of 18 years (P1), 7 years (P2) and 11 years (P3). All patients developed ILD at or within 2 months of diagnosis with dermatomyositis. Patient P1 and P2 developed severe lung disease requiring intubation and extracorporeal membrane oxygenation (ECMO). These two patients were positive for anti-MDA5-ab. Patient P2 had a 1-2 month delay in identification of ILD, and by the time a lung transplant team was consulted, she was too critical to be listed for transplant and ultimately passed away. ILD was identified more rapidly in patient P1, leading to faster treatment with immunosuppression and successful bilateral lung transplant. In contrast, patient P3 tested positive for anti-PM/Scl100 antibody and had features of anti-synthetase-like syndrome, including peeling of the hands and feet. This patient’s lung disease was identified quickly, before the development of respiratory failure. She has responded to treatment with a JAK inhibitor alone and has not required transplant. The other surviving patient was also treated with a JAK inhibitor, whereas the patient who passed away could not tolerate enteral feeding and was never started on JAK inhibition.
Conclusion: Our experience with dermatomyositis-related ILD underscores the importance of early identification and timely referral to lung transplant specialists to avoid delays that can contribute to mortality. Special attention should be paid to the rapidly progressive phenotype that is often seen in dermatomyositis associated with anti-MDA5-ab. These cases illustrate the need for universal ILD screening in all JDM patients regardless of antibody positivity. Furthermore, patients who present with severe lung disease, especially those with anti-MDA5-ab, should be immediately referred to centers with expertise in lung transplant. Lastly, the surviving cases highlight the potential benefit of JAK inhibitor treatment in patients with autoimmune disease-related ILD.
Summary of Patient Characteristics Clinical features of the three dermatomyositis patients, including antibody status, treatments, required respiratory support and outcomes. Abbreviations are used for cyclophosphamide (CYC), plasmapheresis (PLEX), mycophenolate (MYC), rituximab (RITX), tofacitinib (TOF), tacrolimus (TAC), hydroxychloroquine (HCQ).
Clinical features of the three dermatomyositis patients, including antibody status, treatments, required respiratory support and outcomes. Abbreviations are used for cyclophosphamide (CYC), plasmapheresis (PLEX), mycophenolate (MYC), rituximab (RITX), tofacitinib (TOF), tacrolimus (TAC), hydroxychloroquine (HCQ).
Lung Imaging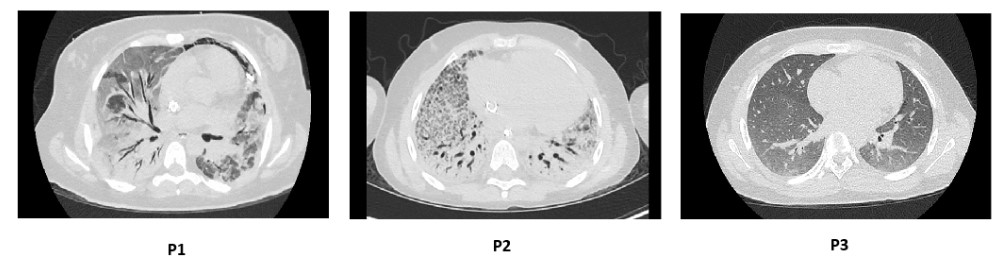 High-resolution Computed Tomography of the Chest demonstrates severe ILD in patient P1 and patient P2, and mild early ILD in patient P3.
High-resolution Computed Tomography of the Chest demonstrates severe ILD in patient P1 and patient P2, and mild early ILD in patient P3.
Pulmonary Function Testing for Patient P3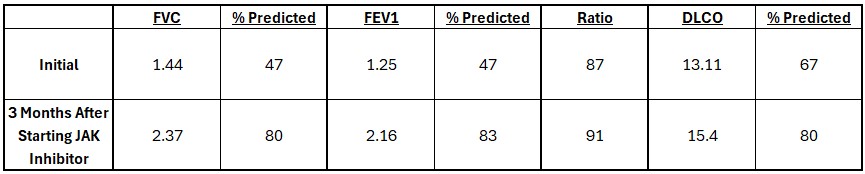 Pulmonary function testing for patient P3 shows improvement in FVC and FEV1 after 3 months of therapy with tofacitinib, hydroxychloroquine, and IVIG. DLCO was normal after correcting for hemoglobin and alveolar volume.
Pulmonary function testing for patient P3 shows improvement in FVC and FEV1 after 3 months of therapy with tofacitinib, hydroxychloroquine, and IVIG. DLCO was normal after correcting for hemoglobin and alveolar volume.
To cite this abstract in AMA style:
Brittain A, Murray E, Stojkic I, Sivaraman V, Krivchenia K, Kirkby S, Akoghlanian S. Lung Transplant for Pediatric Dermatomyositis Patients with Interstitial Lung Disease: A Single-Center Experience [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/lung-transplant-for-pediatric-dermatomyositis-patients-with-interstitial-lung-disease-a-single-center-experience/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/lung-transplant-for-pediatric-dermatomyositis-patients-with-interstitial-lung-disease-a-single-center-experience/