Session Information
Date: Saturday, November 12, 2022
Title: Vasculitis – Non-ANCA-Associated and Related Disorders Poster I: Giant Cell Arteritis
Session Type: Poster Session A
Session Time: 1:00PM-3:00PM
Background/Purpose: Giant Cell Arteritis (GCA) is the most common vasculitis in patients more than 50 years of age in the western countries. Although corticosteroids remain the corner stone of therapy in GCA, we now have other therapeutic options including tocilizumab that was approved by the food and drug administration for GCA in 2017. It is unclear if outcomes of hospitalizations for GCA have changed in recent years following the increased availability of therapeutic options. Long-term longitudinal studies are limited on hospitalizations for GCA. Here we aimed to study longitudinal trends of hospitalizations for GCA in the last 2 decades in the United States (U.S).
Methods: Data were obtained from the National Inpatient Sample database (NIS), the largest hospitalization database in the U.S. We performed a 21-year longitudinal trend analysis of NIS from 1998 to 2018. Every 5th year of the NIS during this study period was sampled. We obtained data from NIS 1998, 2003, 2008, 2013, and 2018 databases. The principal diagnosis is the main reason for hospitalization in the NIS. We searched for hospitalizations for patients aged≥ 50 years with a principal diagnosis of GCA using ICD-9 code “4465” or ICD-10 codes “M315” or “M316”. We used all hospitalizations for adult patients aged ≥50 years as the control population. The primary outcome was longitudinal trends in inpatient mortality of hospitalizations for GCA. Secondary outcomes include longitudinal trends in incidence, hospital length of stay (LOS), total hospital charges, race, gender, age, and Charlson comorbidity index score (CCI). Multivariable logistic and linear regression was used to calculate adjusted p-trend for categorical and continuous outcomes, respectively. We adjusted for changes in demographics and CCI over time. STATA version 16 was used for analysis.
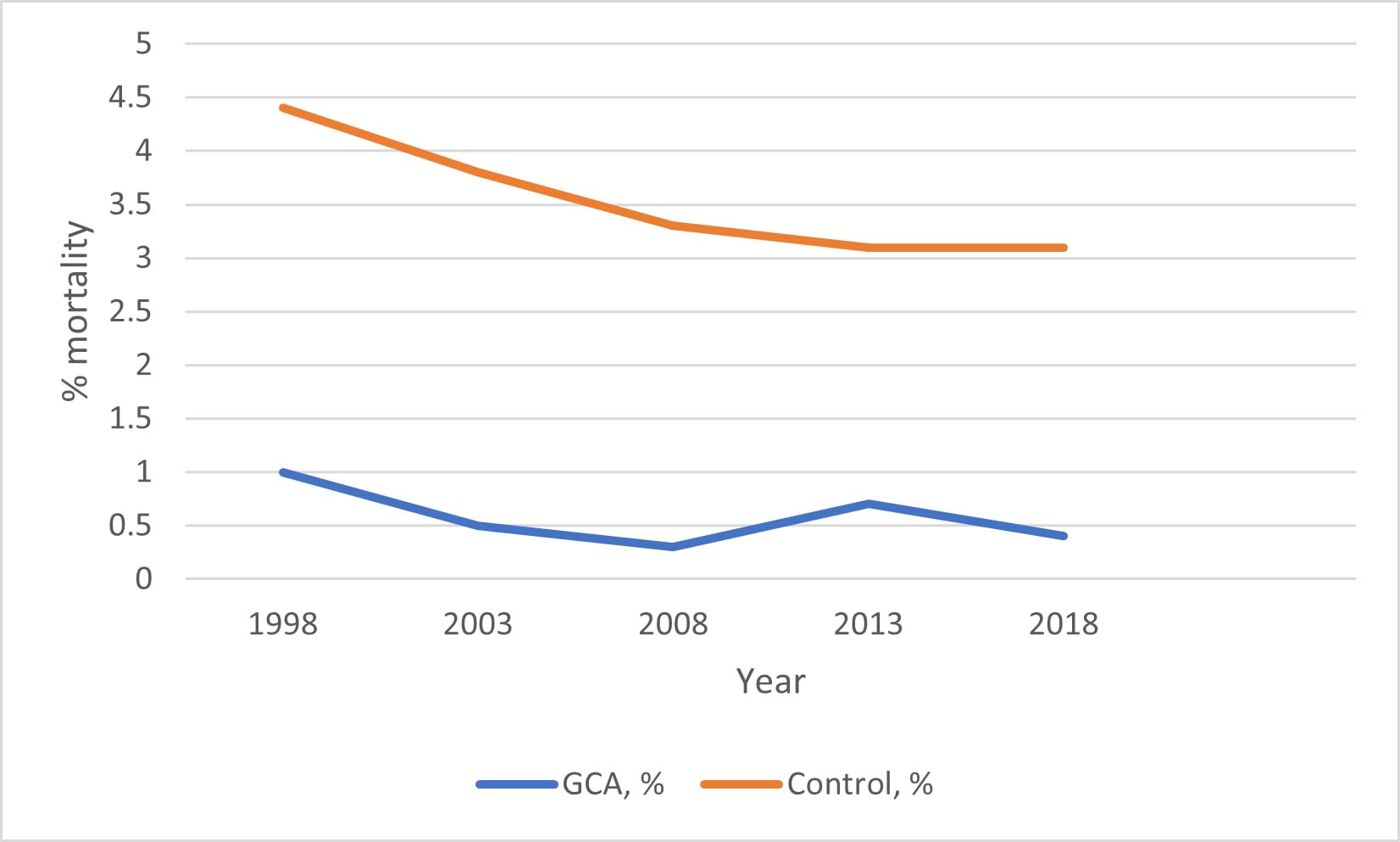
Results: Incidence of hospitalization for GCA remained stable at about 1 per 100,000 US persons throughout the study period. See Table 1. There was no statistically significant change in inpatient mortality for the GCA group during the study period (adjusted p-trend=0.111). In comparison, inpatient mortality reduced from 4.4% to 3.1% from 1998 to 2018 (adjusted p-trend < 0.0001) in the control group. See Figure 1. The proportion of whites reduced, while the proportion of racial minorities increased over time in both the GCA and control groups. There was a statistically significant reduction in the proportion of females and hospital length of stay and an increase in total hospital charges and CCI over time in both groups.
Conclusion: The incidence of hospitalization for GCA has remained stable in the last 2 decades in the U.S. Inpatient mortality of hospitalizations for GCA has not changed significantly compared to the control population which saw a statistically significant reduction in inpatient mortality. Other trends were similar between both groups. Although tocilizumab has been approved as a steroid-sparing agent for chronic GCA management, steroids remain the mainstay of management of acute GCA. More research into different modalities of acute GCA management of hospitalized patients may help in reducing the mortality of these patients.
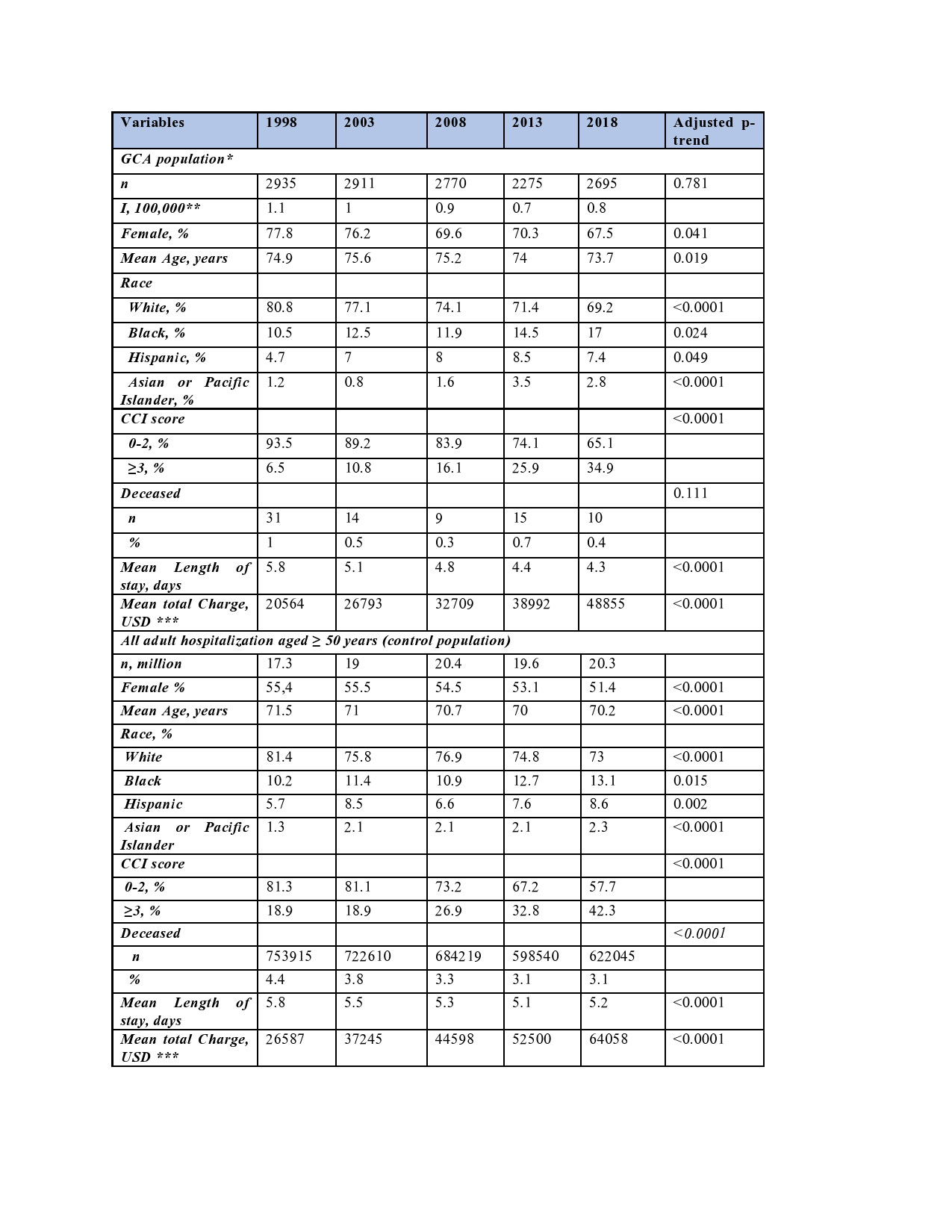
Abbreviations: GCA: Giant cell arteritis, USD: United States Dollars, I: Incidence per 100,000 persons, CCI: Charlson comorbidity index. p<0.005 was statistically significant.
* We included hospitalizations for patients aged ≥50 years with a principal diagnosis of GCA
** The incidence of GCA hospitalizations for GCA was calculated by dividing the number of GCA hospitalizations in the NIS by the population estimate of the U.S on July 1 of the corresponding year. The population estimates were obtained from the U.S Census Bureau Website
*** All hospital charges were adjusted for inflation by using the medical expenditure panel survey-based factor for hospital care and were presented in 2018 United States dollars (USD).
To cite this abstract in AMA style:
Edigin E, Trang A, Anighoro S, Osuorji C, Eseaton P, Idolor O, Hino C, Chukwu N, Hojjati M. Longitudinal Tends of Hospitalizations for Giant Cell Arteritis: A 21-year Longitudinal National Population-based Study [abstract]. Arthritis Rheumatol. 2022; 74 (suppl 9). https://acrabstracts.org/abstract/longitudinal-tends-of-hospitalizations-for-giant-cell-arteritis-a-21-year-longitudinal-national-population-based-study/. Accessed .« Back to ACR Convergence 2022
ACR Meeting Abstracts - https://acrabstracts.org/abstract/longitudinal-tends-of-hospitalizations-for-giant-cell-arteritis-a-21-year-longitudinal-national-population-based-study/