Background/Purpose: Takayasu’s Arteritis (TAK) is a chronic inflammatory large vessel vasculitis characterized by granulomatous inflammation of the aorta and its branches. TAK incidence is 2.6/million annually in Minnesota. Prevalence is higher in Asian and Indian populations. TAK predominantly affects younger woman under 40 years of age. Renal artery involvement (RAI) in TAK is a poor prognostic factor. However, long-term outcomes of TAK patients with RAI have not been reported.
Methods: We performed a retrospective chart review of 37 patients from Addenbrooke’s Hospital, UK, and 13 patients from Skane University Hospital, Sweden. Diagnosis of TAK was based on the presence of constitutional symptoms, elevated inflammatory markers, and vascular abnormalities on angiography. RAI was identified based on conventional, CT or MR angiography. Data was collected on patient demographics and presenting symptoms, signs, co-morbidities, blood pressure and medications. Laboratory values including creatinine, erythrocyte sedimentation rate, and c-reactive protein were collected. Disease activity was assessed using the Indian Takayasu Activity Index 2010 (ITAS2010). Irreversible organ damage was assessed using the vasculitis damage index (VDI). Worsening or improved renal function was defined as a drop or increase in eGFR > 20%.
Results: Sixteen of 50 (32%) TAK patients were identified to have RAI. Presenting demographics and disease parameters are summarized in Table 1. Two patients had structural renal disease (PUJ obstruction and prior renal surgery undefined) and are among the 7 patients with renal asymmetry; one was among the nine patients with pre-existing hypertension. The three with eGFR <60 ml/min had moderate renal dysfunction (eGFRs of 45, 57, and 59 ml/min).

Follow-up data is presented in Table 2. Median follow-up duration was 8.8 years (10 months – 30 years). Among the 13 with hypertension including two who developed hypertension over the follow-up period; 11 were on anti-hypertensive drugs. Among the six patients with renal asymmetry; five were known and one developed this over the follow-up period. Among those with eGFR < 60 ml/min at presentation, one improved, one declined (patient with PUJ obstruction), and one remained stable.
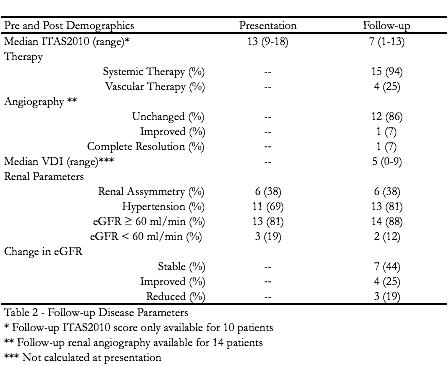
Conclusion: The prevalence of RAI in this population (32%) is comparable to that in the literature. Hypertension was common. Most patients had normal eGFRs, despite severe disease. Disease progression was minimal. Our results suggest renal prognosis is better than previously thought.
Disclosure:
C. Baldwin,
None;
A. Mohammad,
None;
D. Jayne,
None.
« Back to 2014 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/long-term-outcomes-of-takayasus-arteritis-patients-with-renal-artery-involvement/