Session Information
Date: Monday, November 11, 2019
Title: Pediatric Rheumatology – ePoster II: SLE, Juvenile Dermatomyositis, & Scleroderma
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: Steroid use in Kawasaki disease (KD)is controversial and has swung from contraindicated, to maybe & now perhaps “should be given to all.”(1) Currently, standard practice is to use IVIg for all children with KD and add upfront steroids to IVIg only for those children who are at risk of non- response to IVIg , if such children can be identified. (2) There is data to support the use of steroids at 2mg/kg/day as an add on to IVIg for the child who is at high risk of non response to the 1st IVIg (3) At our center, over the last 18 years we have observed1. significant no. of children present with CALs & 2. These children often do not respond to 1st dose of IVIG. Thus, from 2017 we changed our practice & added steroids to IVIG as an upfront therapy to children presenting with CALs. We audited our practice & present the data on 65 children with KD.
Purpose:
- To study demographic & clinical profile of children with KD.
- To study response rate of IVIg
- To study the difference in response rate (if any ) for the child with KD & CALs who was given only IVIg ( pre 2017) or IVIg & steroids ( post 2017) at first presentation
Methods: All children diagnosed with KD from Jan13 to Apr19 were included. Clinical & demographic details were recorded on predesigned proformas. CALs were defined by z score (Boston) of more than 2 in any coronary artery. Response to IVIG was defined as no fever 36 hours post IVIG completion. Patients given IVIG alone got high dose aspirin, with steroids only low dose was given.SPSS 17.0 was used for analysis.
Results: 65 KD patients reviewed. Clinical & demographic details in Table 1. CALs were present in 31(47.6%) children at diagnosis. Boys had more CALs at onset than girls(p=0.059) IVIg was given to all. Steroids as first line were given to 13(20%): All had CALs. A second dose of IVIG was required by 13(20%). Therapy detailed in Table 2. IVIg alone had a poor response in those presenting with CALs. Addition of steroids to IVIG upfront was associated with significant increase in response in those with CALs(p=0.001) Details in table 3. No factors predicted the response to IVIG alone(age, day of diagnosis, C reactive protein). A higher z score predicted poor response to IVIG alone(p< 0.005), thus reiterating the fact that steroids are helpful in KD patients with CALs Kawasaki shock syndrome was seen in 2(3%) and macrophage activation syndrome in 1(1.5%),requiring high dose methylprednisolone(10-30mg/kg/day). At median follow up of 14 months(IQR 8-15), CALs normalized in 27(86%),5 persisted to have abnormal CALs. ( All had giant aneurysms at presentation, Z scores >10). There was no mortality in this cohort.
Ref:
- Corticosteroids for the treatment of KD in children. Cochrane Review 2017.
- Diagnosis, Treatment, and Long-Term Management of KD. 2017.
- Efficacy of IVIG plus prednisolone for prevention of CALs in severe Kawasaki disease (RAISE study): Lancet 2012
Conclusion:
- 47% KD patients presented with CALs.
- KD with CALs have poor response to IVIG alone vs IVIG with upfront steroids (p=0.001)
- In addition to the well described scoring systems that predict a poor response to IVIG in the Japanese population, the presence of CALs and risk of non response to IVIG needs further study and replication in cohorts across the world.

table 1

table 2
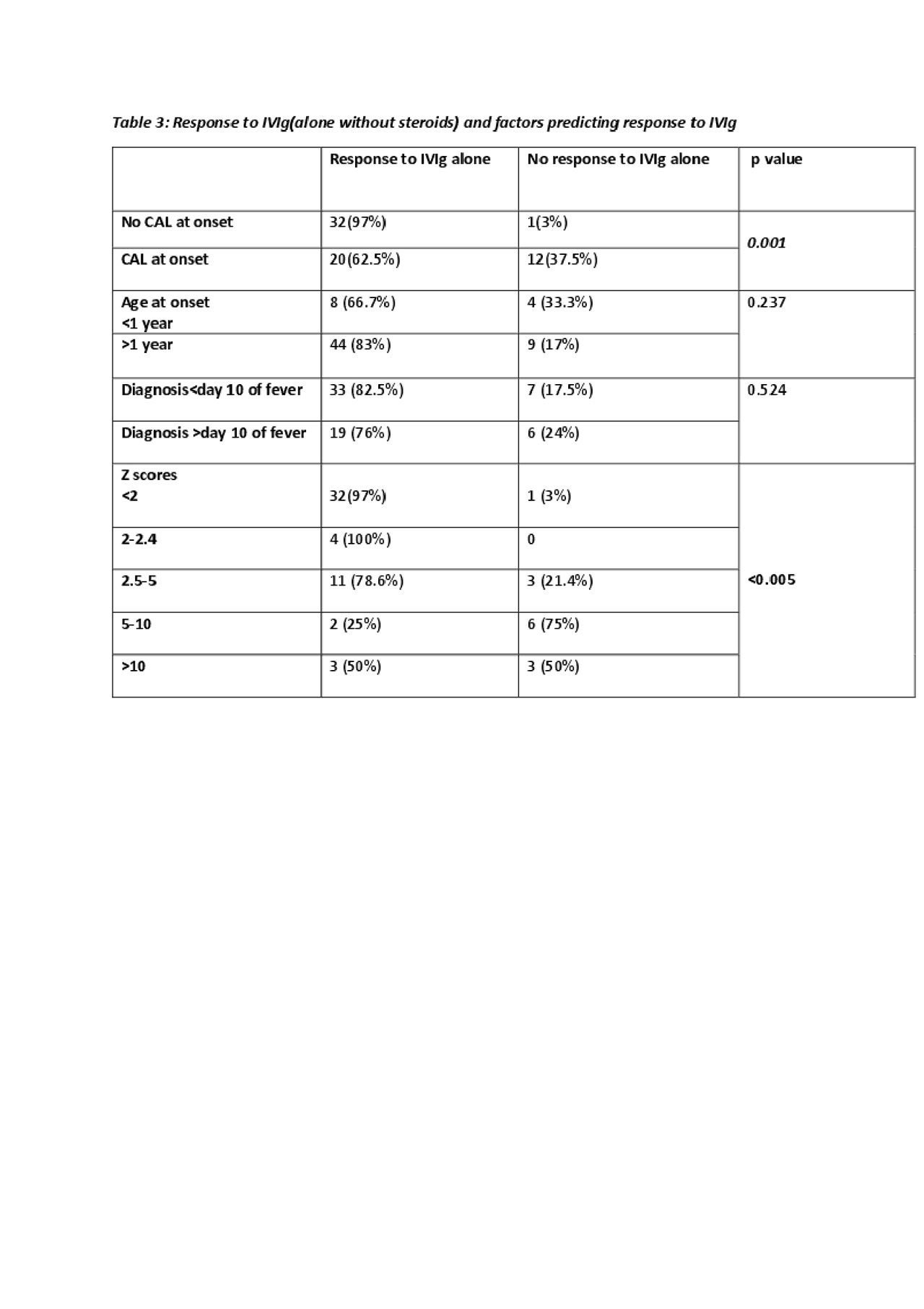
table 3
To cite this abstract in AMA style:
Agarwal M, Mittal S, Singh A, Agarwal N, Sawhney S. Kawasaki Disease: Is Intravenous Immunoglobulin Alone Adequate for the Child with Kawasaki Disease and Coronary Artery Lesions? A Retrospective Study of 65 Children with Kawasaki Disease from a Single North Indian Centre [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/kawasaki-disease-is-intravenous-immunoglobulin-alone-adequate-for-the-child-with-kawasaki-disease-and-coronary-artery-lesions-a-retrospective-study-of-65-children-with-kawasaki-disease-from-a-single/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/kawasaki-disease-is-intravenous-immunoglobulin-alone-adequate-for-the-child-with-kawasaki-disease-and-coronary-artery-lesions-a-retrospective-study-of-65-children-with-kawasaki-disease-from-a-single/