Session Information
Session Time: 5:00PM-6:00PM
Background/Purpose: Macrophage activation syndrome (MAS) is a rare, life-threatening complication seen in rheumatic disease that requires timely identification and rapid treatment. While MAS is best recognized and most commonly seen with systemic juvenile idiopathic arthritis (sJIA), emerging literature emphasizes the risk of MAS development among patients with juvenile idiopathic inflammatory myopathies (IIMs). To date, there is limited available literature investigating potential trends among patients with juvenile IIMs who develop MAS. This single-center case series provides insight into potential trends to consider whenmonitoring patients with juvenile IIM for risk of MAS development.
Methods: A retrospective chart review was conducted at a single large quaternary center using ICD-10 codes for juvenile IIM (M33.0, M33.2, G72.4) in the electronic medical record to identify patients with juvenile IIMs and macrophage activation syndrome (D76.1) between 1/1/2009 and 12/1/2024. In our search, our patients’ MAS episodes occurred between 2009 and 2024. Patients with normal ferritin (< 100ng/mL) or lack of fever on review were excluded. Descriptive statistics and a review of the literature on juvenile IIM and MAS were completed.
Results: Of 123 patients with juvenile IIMs followed at our center 16 patients were screened with ICD-10 codes and on further detailed review, 10 patients were included in this series as having MAS diagnosed by a pediatric rheumatologist, 5 of whom required admission to the intensive care unit. Eight of the ten patients were diagnosed with MAS at or near IIM diagnosis, whereas two patients were diagnosed 13 and 15 years after IIM onset. Age of IIM onset ranged from 2-17 years old, and range of MAS onset was also 2-17 years old, with a bimodal distribution (Figure 1). Median creatinine kinase was 2498 IU/L (range 57-30176 IU/L), median ferritin was 2655 ng/mL (range 429-9720 ng/mL), and median platelets were 142 k/mm3 (range 8-461 k/mm3). Twenty percent of patients met hemophagocytic lymphohistiocytosis (HLH) 2004 criteria, whereas eighty percent of patients met the 2016 sJIA-MAS criteria. There were a variety of myositis specific antibodies including three patients with anti-MJ (NXP2), two of whom were admitted to the ICU, two with anti-P155/140 (TIF-1- γ), two with anti-MDA5, one patient with anti-JO1, and two without identified myositis autoantibodies (Table 1). Treatment included corticosteroid pulses for all ten patients, anakinra for six of the ten patients, cyclosporine for two patients, cyclophosphamide for one patient, and one did not require additional immune suppressant therapy beyond steroids. Seven patients were started on IVIG as part of their IIM maintenance therapy around the time of their MAS, and another had recently received cyclophosphamide prior to their MAS episode.
Conclusion: Patients with juvenile IIMs are at risk of MAS and diagnosis requires a high index of suspicion. Patients in our cohort with MAS had lower ferritins and relative thrombocytopenia with good response to therapies like anakinra and steroid pulses. MAS with juvenile IIM may present differently than SJIA-associated MAS and is likely underrecognized.
Figure 1. 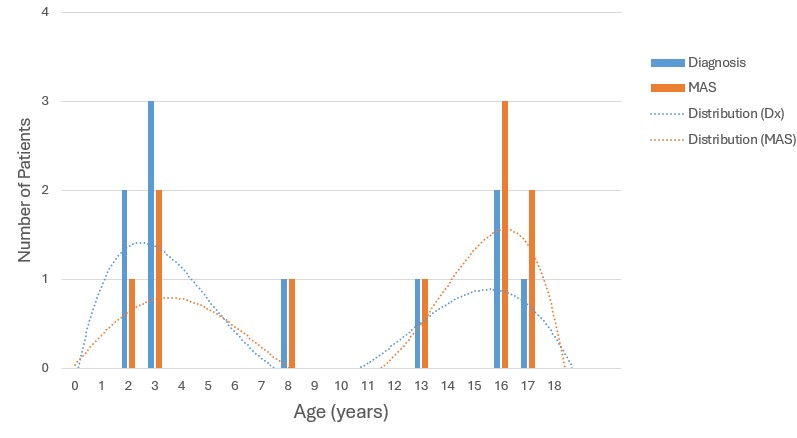 Figure 1. Distribution of age at diagnosis and at macrophage activation syndrome onset. Bars indicate number of patients at each age in years. Dotted lines indicate distribution of patients. MAS=Macrophage activation syndrome; Dx=Diagnosis
Figure 1. Distribution of age at diagnosis and at macrophage activation syndrome onset. Bars indicate number of patients at each age in years. Dotted lines indicate distribution of patients. MAS=Macrophage activation syndrome; Dx=Diagnosis
Table 1.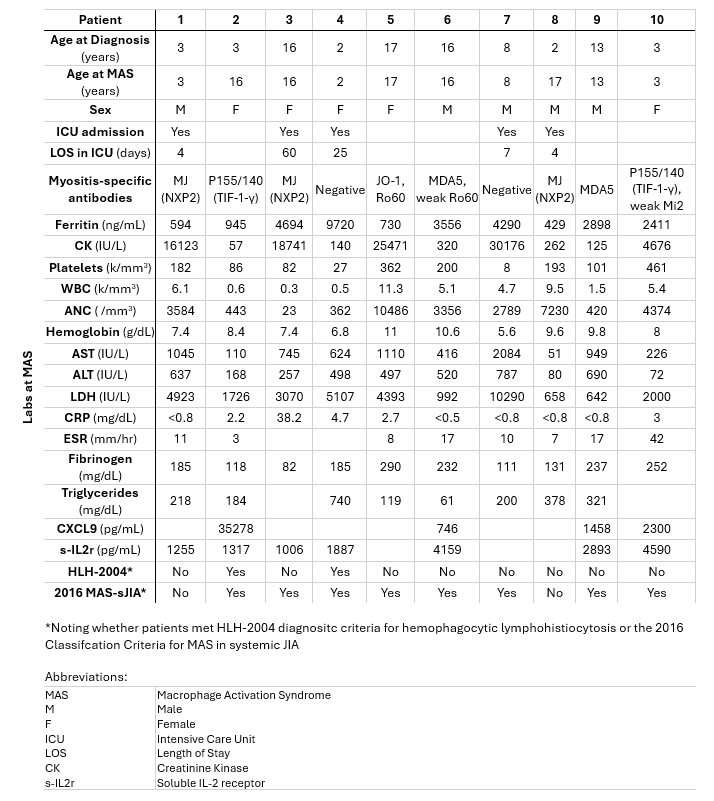 Table 1. Demographics for patients with IIM and MAS. IIM=Idiopathic inflammatory myopathy; MAS=Macrophage activation syndrome
Table 1. Demographics for patients with IIM and MAS. IIM=Idiopathic inflammatory myopathy; MAS=Macrophage activation syndrome
To cite this abstract in AMA style:
Moussouras N, Levy A, Shenoi S. Juvenile Idiopathic Inflammatory Myopathies and Macrophage Activation Syndrome: A Case Series [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/juvenile-idiopathic-inflammatory-myopathies-and-macrophage-activation-syndrome-a-case-series/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/juvenile-idiopathic-inflammatory-myopathies-and-macrophage-activation-syndrome-a-case-series/