Session Information
Session Time: 6:00PM-7:00PM
Background/Purpose: Early diagnosis and treatment of Juvenile Idiopathic Arthritis (JIA) minimizes the accrual of joint damage and improves long-term outcomes. However, many patients with JIA experience a prolonged, circuitous path to diagnosis. This study explores the experiences of caregivers of patients with JIA during the diagnostic journey to identify common patterns and experiences and to create journey maps of the diagnostic process.
Methods: We utilized semi-structured qualitative interviews with caregivers of children diagnosed with JIA between 2023 and 2025. Interviewees were purposively sampled from patients with short (<10 weeks, n=10), medium (10-24 weeks, n=10) or long ( >24 weeks, n=10) time to diagnosis. Using NVivo for data coding and an inductive analysis approach, we identified common patterns and experiences of the journey to JIA diagnosis, exploring variation across comparison groups. We generated journey maps (Figure 1) as an analytic strategy, guiding theme development and allowing for cross-case comparison.
Results: Interviewees (n=30, Table 1) reported that early symptoms, like non-specific joint pain, were often interpreted by parents and clinicians as sports-related trauma, overuse injuries, or growing pains. Once children exhibited joint swelling or functionally limiting symptoms, such as limping, there was an inflection point in the diagnostic process; parents experienced heightened concern and presented for more care. It often required multiple visits for parental concern to converge with clinician concern, and frequently multiple providers were seen before JIA was considered as a possible diagnosis. The most common provider types seen were primary care providers, emergency department/urgent care providers, and orthopedists. Common patterns identified in cases with a more prolonged path to diagnosis included (1) minimization of symptoms by caregivers, (2) non-specific symptoms or waxing and waning symptoms that overlap with other common childhood conditions, (3) lack of provider familiarity with inflammatory arthritis or provider dismissiveness of parental concerns, and (4) scheduling delays. Common patterns identified in cases with a more direct path to diagnosis included (1) parental advocacy and perseverance, (2) factors that resulted in ease of accessing care and scheduling appointments, and (3) familiarity with autoimmune conditions (Table 2). Interviewees reported they might have sought care more urgently if they had known about JIA and that many clinicians seem to lack awareness of JIA.
Conclusion: Patients with JIA often experience prolonged, indirect paths to diagnosis. This circuitous diagnostic journey is likely multifactorial with contributions from minimization of symptoms by caregivers, non-specific symptoms that overlap with more common conditions, lack of clinician familiarity with the condition, and scheduling delays. We have generated representative journey maps of archetypal diagnostic trajectories. Increased awareness of early signs and symptoms of JIA amongst caregivers and clinicians could facilitate a more timely, direct diagnostic path and earlier referral to rheumatology.
Cohort Demographics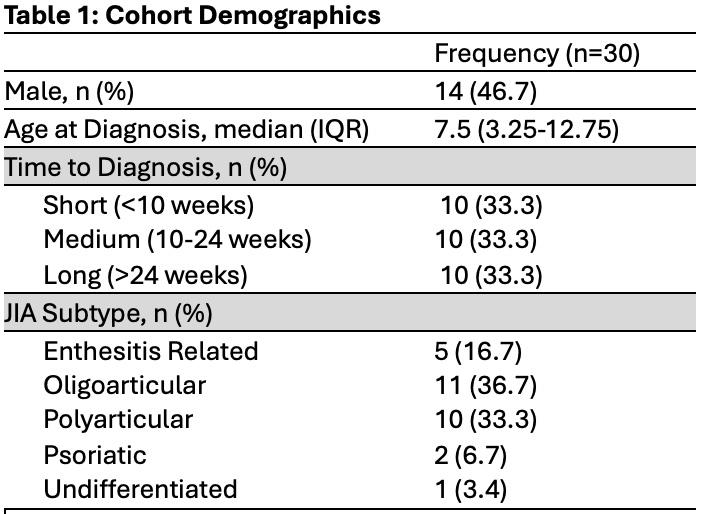
Figure 1: Diagnostic Journey Map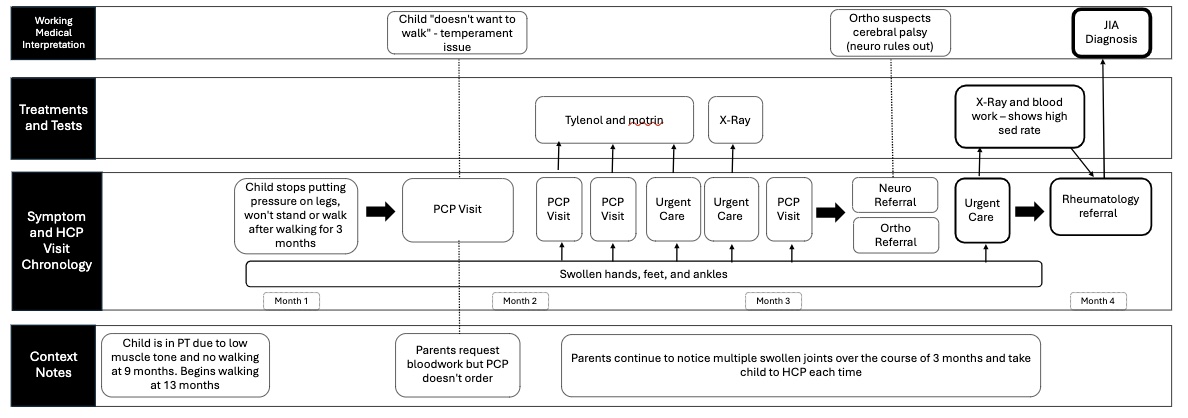
Table 2: Common Patterns with Representative Quotes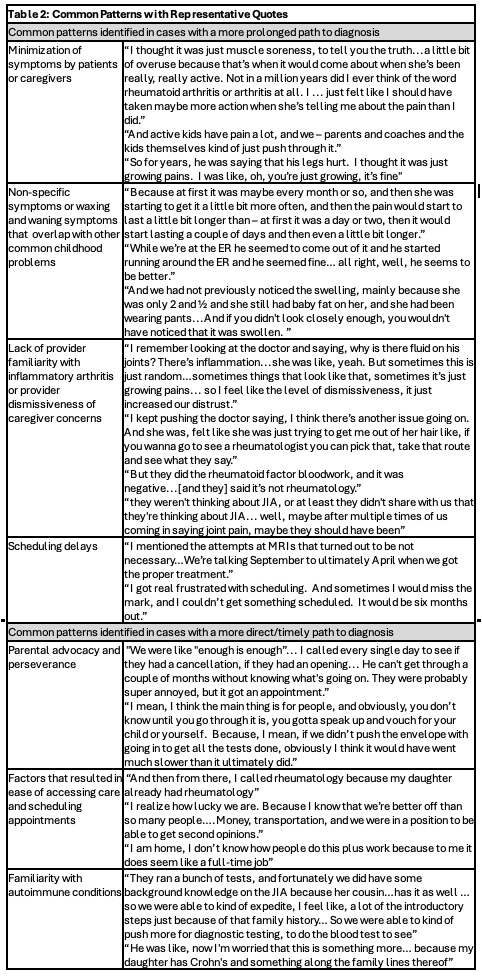
To cite this abstract in AMA style:
Anna C, Chatterjee A, Quzack L, Meyer A, Jazayeri J, Kaur A, Weiss P, Kellom K, Rasooly I. Journey Maps of the Diagnostic Process: Insights from Caregivers of Patients with Juvenile Idiopathic Arthritis [abstract]. Arthritis Rheumatol. 2026; 78 (suppl 3). https://acrabstracts.org/abstract/journey-maps-of-the-diagnostic-process-insights-from-caregivers-of-patients-with-juvenile-idiopathic-arthritis/. Accessed .« Back to 2026 Pediatric Rheumatology Symposium
ACR Meeting Abstracts - https://acrabstracts.org/abstract/journey-maps-of-the-diagnostic-process-insights-from-caregivers-of-patients-with-juvenile-idiopathic-arthritis/