Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Juvenile SpA (JSpA) involve enthesitis related arthritis (ERA), juvenile psoriatic arthritis and undifferentiated arthritis (UA) according to the ILAR criteria. Two different patterns have been found: axial and peripheral. The pediatric form differs from that in adults by a predominant peripheral involvement. The evolution to ankylosis has been reported in one third of all cases after several years. The proposed PRINTO classification criteria for JIA introduced a new approach changing ERA to enthesitis/spondylitis-related JIA (ESRA) resulting in a definition harmonized with that for adults. The purposes were to assess the sensibility and specificity of the provisional new PRINTO JIA classification criteria for ESRA and to compare its performance to others adult´s classification criteria. To identify predictive variables for ankylosis progression.
Methods: Consecutive patients with JSpA (defined as ERA or UA according to ILAR) followed in our center were included. Randomly selected patients with oligoarthritis (23), polyarthritis RF negative (22) and systemic (20) served as controls. Variables recorded included: arthritis, enthesitis, tarsitis, inflammatory back pain (IBP), SI- joint tenderness, presence of HLA-B27 antigen, acute anterior uveitis, history of SpA in a first-degree relative. Imaging on SI-joints (SI joints) on X-ray and/or MRI. Classification criteria for adults were ASAS and Modified New York (NY). Patients with ankylosing progression fulfilled NY criteria. Summary statistics: sensitivity, specificity, positive predictive value (PPV), negative predictive value (NVP), positive Likelihood ratio (+LR) and negative Likelihood ratio (-LR). Univariate and multivariate logistic regression for predictors variables.
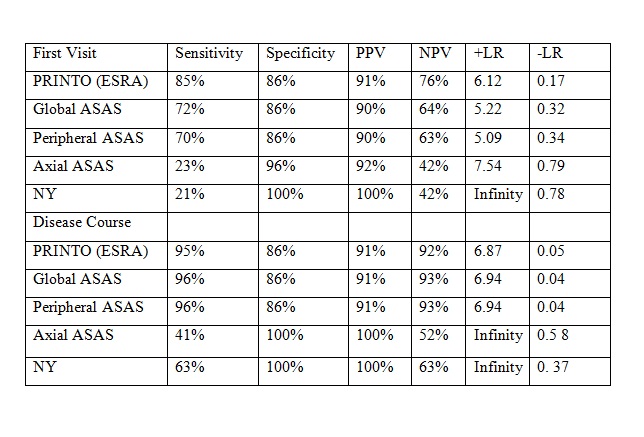
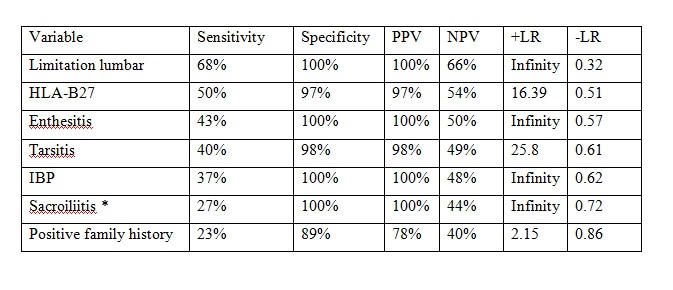
Results: 112 patients with JSpA (89 ERA, 23 UA) were included (M: 94), median age at onset: 10 (1-15) years, disease duration at time of first visit 8.5 (1-48) months, follow-up 7 (1-15) years. Controls: 65 JIA (M: 27). At first visit showed: 107 (95%) arthritis, 69 (62%) elevated CRP, 54 (48%) limitation of lumbar spine motion, 56 (50%) HLA-B27, 48(43%) enthesitis, 44 (40%) tarsitis, 42 (37%) IBP, 31 (30%) SI- joint tenderness, 30 (27%) good response to NSAIDS, 26 (23%) positive family history, 12 (10%) dactylitis, 7(6%) uveitis,7(6%) diarrhea, 5(5 %) infectious previous, 2(2%) urethritis, 2(2%) IBD, 2 (2%) buttock pain. Imaging for sacroiliitis: 30 (27%) on X-Ray (23 grade 2 bilateral and 7 grade 3), 26 (23%) on MRI. At first visit (112 patients): 95 (87%) fulfilled ESRA criteria. Disease course (102 patients): 97 (95%). Patients who meet NY criteria: 64 (63%). Table 1 shows the accuracy for classification criteria. The unique predictor variable for ankylosing progression was lumbar limitation (p=0.02). Table 2 shows the accuracy of the selected variables at onset of the disease for predicting the risk of developing JAS.
Conclusion: The new proposed PRINTO criteria was a more sensitive classification criteria than adults’ criteria. Lumbar limitation was a predictor variable for ankylosing. The accuracy of each selected variable at onset suggests the probability of a higher suspected index for JSpA.
To cite this abstract in AMA style:
Katsicas M, Bertinotti M, Villarreal M. Is There a Need for a New Classification Criteria in Juvenile Spondyloarthritis? [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/is-there-a-need-for-a-new-classification-criteria-in-juvenile-spondyloarthritis/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/is-there-a-need-for-a-new-classification-criteria-in-juvenile-spondyloarthritis/