Session Information
Session Type: Poster Session (Monday)
Session Time: 9:00AM-11:00AM
Background/Purpose: In Familial Mediterranean Fever (FMF), patients having exon 10 mutations, specifically M694V, M680I, and V726A are more common and their disease profiles tend to complicate more. Hence, among the 10 exons of the MEFV gene, the association between FMF and these mutations are well known. Other mutations, especially the ones in exon 2, can be defined as benign polymorphisms due to being rare. The objective of this study was to understand the clinical nature of patients having mutations of E148Q and R202Q in exon 2 as well as how these mutations affect their complaints and treatment response.
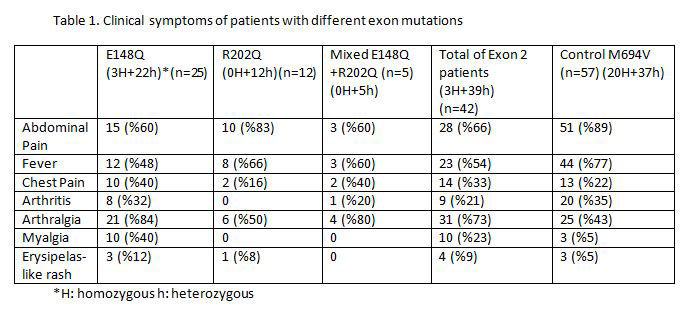
Methods: In this study, we reported patients with FMF diagnosis according to Tel Hashomer criteria, who had mutations of E148Q, R202Q or both. These patients were a randomized subset of the ones followed in our outpatient rheumatology clinic. Clinical features of these patients were collected from their files. In terms of symptoms abdominal pain, chest pain, fever, arthritis, arthralgia, myalgia, erysipelas-like rash were noted. In terms of complications, renal FMF-related systemic AA Amyloidosis was noted. Also, we checked the family history of FMF. These patients were compared with the control group of patients having M694V mutation. M694V was selected as the control group because this mutation is well known scientifically and is the most frequent among FMF patients.
Results: The clinical symptoms of the patients are summarized in Table 1. One of the primary outcomes of this study was the treatment response. 98% of the patients were treated with colchicine when they were diagnosed with FMF. Fifty-two patients (91%) responded to colchicine in the control group whereas 33 (78%) responded to colchicine in Exon 2 group. To further digest the exon 2 patients, all of the patients in the R202Q group, 68% of the E148Q group, and 80% of the mixed exon 2 group responded to colchicine. Family history was positive in 9 patients (36%) of E148Q group, in 1 patient (8%) of R202Q group, in 1 patient (20%) in mixed exon 2 group which equals a total of 11 patients (26%). In the control group, 39 patients (68%) had an FMF diagnosis in their family. Amyloidosis was reported in one patient with E148Q mutation, one patient with R202Q mutation, two patients with M694V mutation.
Conclusion: In conclusion, in comparison with M694V patients, patients with exon 2 mutations, tend to have more atypical symptoms of FMF such as chest pain, arthralgia, and myalgia. The presentation of these symptoms is milder than the typical symptoms of FMF. The fact of low colchicine response in exon 2 patients cannot be overlooked as well. Therefore, exon 2 mutations can be evaluated as a separate clinical entity; in fact, these cases should also be further searched for a potential autoinflammatory disorder.
To cite this abstract in AMA style:
Kulaksiz B, Egeli B, Aydin O, Ugurlu S. Is Exon 2 Associated with FMF or a New Disease? [abstract]. Arthritis Rheumatol. 2019; 71 (suppl 10). https://acrabstracts.org/abstract/is-exon-2-associated-with-fmf-or-a-new-disease/. Accessed .« Back to 2019 ACR/ARP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/is-exon-2-associated-with-fmf-or-a-new-disease/