Session Information
Session Type: ACR Poster Session C
Session Time: 9:00AM-11:00AM
Background/Purpose: ANCA-associated vasculitis (AAV) is a group of rare systemic vasculitidies with significant morbidity and mortality. There have been no comparative effectiveness studies of AAV in children. We aimed to determine if use of plasma exchange (PLEX), in addition to standard immunosuppression, was associated with a decreased need for dialysis among children hospitalized with AAV.
Methods: We used the Pediatric Health Information System (PHIS) database to conduct a retrospective cohort study of children hospitalized with AAV from 2004-2014. PHIS contains inpatient administrative and billing data from 47 hospitals in the United States. Patients with the ICD-9-CM code 446.4 as one of the discharge diagnoses and ≥1 charge for glucocorticoids were included. Patients who underwent a renal transplant during their first hospitalization were excluded. We used multivariate mixed effects logistic regression models accounting for clustering by hospitalization to determine if initiation of dialysis within 6 months of the first admission was associated with use of PLEX within the first 7 days (primary exposure) or use of cyclophosphamide (CYC) or rituximab during the first admission. For regression modeling, patients initiating dialysis within the first 3 days of hospitalization were excluded (N= 36). We adjusted for intensive care unit (ICU) stay in the first 24 hours as a proxy for disease severity.
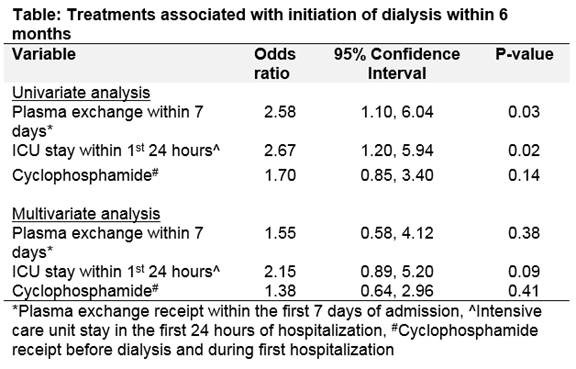
Results: During the study period there were 1284 admissions for 389 children with AAV, 78 (20%) of whom required dialysis at some point during the study period. Median age at first admission was 14.7 years (interquartile range (IQR) 12.2, 16.1) and 61% were female. Median time to initiation of dialysis was 3 days (IQR 1, 21); 68 (87%) patients started dialysis within 6 months of initial hospitalization. Twenty-five (6%) patients received a renal transplant at a median of 20.6 months (IQR 11.5, 26.4) after first admission. No patients received a renal transplant before initiation of dialysis. Of the 32 patients receiving dialysis included in the regression model, 60 % were female, with a median age of 13.7 years (IQR 10.8, 15.4), 14 (44%) had ICU admissions in the first 24 hours, and 25%, 65%, and 9% received PLEX, CYC , or rituximab, respectively, prior to dialysis. PLEX and ICU stay in the first 24 hours were significantly associated with increased odds of needing dialysis within 6 months in univariate, but not multivariate analysis (Table). CYC use was not associated with an increased or decreased likelihood of dialysis in univariate or multivariate analysis. Associations with rituximab could not be determined due the rarity of its use before dialysis.
Conclusion: Twenty percent of children hospitalized with AAV require dialysis with the vast majority initiating dialysis within 6 months of their first admission for AAV. Neither use of PLEX, nor use of CYC is associated with initiation of dialysis within 6 months in children with AAV.
To cite this abstract in AMA style:
James K, Xiao R, Merkel PA, Weiss PF. Initiation of Dialysis in Pediatric ANCA-Associated Vasculitis [abstract]. Arthritis Rheumatol. 2016; 68 (suppl 10). https://acrabstracts.org/abstract/initiation-of-dialysis-in-pediatric-anca-associated-vasculitis/. Accessed .« Back to 2016 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/initiation-of-dialysis-in-pediatric-anca-associated-vasculitis/