Session Information
Session Type: Poster Session A
Session Time: 8:30AM-10:30AM
Background/Purpose: Eosinophilic granulomatosis with polyangiitis (EGPA), formerly Churg-Strauss Syndrome, is a rare, complex multisystem disorder, characterized by vascular inflammation and multisystem organ damage. EGPA manifests as asthma, chronic rhinosinusitis, blood/tissue eosinophilia, and vasculitis. In part due to its rare nature, there is an absence of real-world data quantifying the healthcare cost of EGPA. This study aims to quantify the incremental healthcare resource utilization (HRU) and costs associated with EGPA as compared to asthma using commercial insurance claims data in the United States (US).
Methods: A retrospective analysis was conducted using the IQVIA PharMetrics Plus Database identifying patients (pts) diagnosed with EGPA between 30 September 2008 and 01 October 2018. Prior to the implementation of ICD-10, EGPA diagnosis was based on published ICD-9-based algorithms.1,2 Post October 2015, EGPA diagnosis was based on ICD-10 code M30.1 (polyarteritis with lung involvement [Churg-Strauss]). The first observed ICD-9/10 claim for EGPA was the index date. An asthma control cohort (ICD-9: 493.X; ICD-10: J45.X) was also identified (date of first asthma claim = index date). Pts in both cohorts were ≥18 years of age with continuous health plan enrollment (6-months pre- and 12-months post-index). Pts in the EGPA cohort were matched to pts in the asthma cohort (matching ratio 1:5) using direct covariate matching (age at index, year of index, gender, geographic region, and Charlson-Comorbidity Index [CCI] score). Results are reported as counts, percentages and means (standard deviation [SD]). Multivariable analysis was conducted to estimate adjusted total, all-cause costs using a generalized linear model (GLM). Statistical comparisons were evaluated at α=0.05 level.
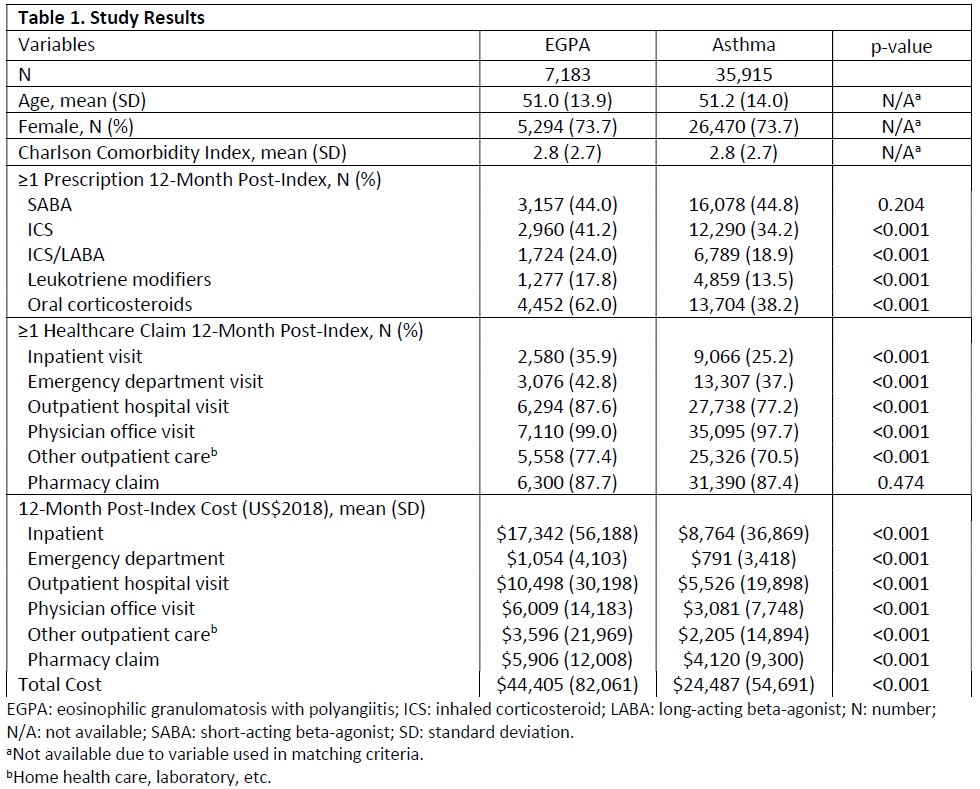
Results: After matching, the EGPA and asthma cohorts consisted of 7,183 and 35,915 pts, respectively. Based on covariate matching, the cohorts were similar in terms of baseline characteristics (mean age: 51 years; 73% female; mean CCI score: 2.8) (Table 1). In the 12-month post-index period, significant differences between the EGPA and asthma cohorts were observed (Table 1) for the following: (1) proportion of pts with asthma-related medication (with exception of short-acting beta-agonists), (2) proportion of pts with ≥1 HRU claim by setting of care (with exception of pharmacy claims); and (3) mean total costs and costs by setting of care. Unadjusted total costs in the 12-month post-index period were $44,404 (82,060) and $24,487 (54,691) in the EGPA and asthma cohorts, respectively (p< 0.001). Adjusted total costs in the 12-month post-index period were $34,004 in the EGPA cohort and $19,552 in the asthma cohort (rate ratio: 1.74; 95% confidence internal: 1.68, 1.79; p< 0.001).
Conclusion: In the 12-month post-index period, HRU and costs were significantly higher for EGPA patients than asthma pts. This study demonstrates the incremental burden of EGPA and highlights the need for effective treatments that reduce the burden of disease and improve patient outcomes.
1Sreih et al. Pharmacoepidemiol Drug Saf 2016;25:1368-74.
2Harrold et al. Pharmacoepidemiol Drug Saf 2004;13:661-7.
To cite this abstract in AMA style:
Bell C, Meyers J, Ajmera M. Incremental Healthcare Costs of Eosinophilic Granulomatosis with Polyangiitis (EGPA) Compared to Asthma: Retrospective Analysis of Commercial Claims Data in the United States (US) [abstract]. Arthritis Rheumatol. 2021; 73 (suppl 9). https://acrabstracts.org/abstract/incremental-healthcare-costs-of-eosinophilic-granulomatosis-with-polyangiitis-egpa-compared-to-asthma-retrospective-analysis-of-commercial-claims-data-in-the-united-states-us/. Accessed .« Back to ACR Convergence 2021
ACR Meeting Abstracts - https://acrabstracts.org/abstract/incremental-healthcare-costs-of-eosinophilic-granulomatosis-with-polyangiitis-egpa-compared-to-asthma-retrospective-analysis-of-commercial-claims-data-in-the-united-states-us/