Session Information
Date: Monday, November 9, 2020
Title: Vasculitis – Non-ANCA-Associated & Related Disorders Poster II
Session Type: Poster Session D
Session Time: 9:00AM-11:00AM
Background/Purpose: To investigate real life glucocorticoid (GC) dosing and relapse rates in patients with new onset giant cell arteritis (GCA) in a single center.
Methods: Complete clinical data taken from the inpatient and outpatient records of consecutive GCA patients followed beyond stopping GC were retrospectively analyzed for GC doses, other immunomodulatory agents and relapses. We excluded patients with incomplete follow-up, in interventional trials and on tocilizumab treatment. All patients consented to anonymous workup of their data, which was approved by the local ethics committee.
Results: 55 patients with GCA (71% female, age 71.4±10.2 (mean±SD) years), diagnosed by biopsy or FDG-PET were included. Of these, 24 (42%) patients relapsed. Methotrexate treatment was not significantly associated with fewer relapses. Of the 31 patients without relapse, one had additional GCs because of another condition. From the prednisolone equivalent data of the remaining 30 patients we calculated 25%, 50% and 75% quartiles. Patients were grouped according to prednisolone start doses of ≤100 mg (standard dose, n=17) and >100 mg (pulse, n=13). In the 25% percentile, patients reached a dose of 15 mg or lower at days 40 (standard) and 49 (pulse), of 7.5 mg prednisolone or lower on day 169 (after 24 weeks) in either arm, and were off prednisolone on days 496 (70 weeks) and 546 (78 weeks) for low dose and high dose start, respectively. Four of the 24 patients with relapses had relapsed after stopping prednisolone clearly (17 to 58 weeks) earlier than the 25% quartile. Of the 20 other patients with relapses, only one was distinctly ( >10%) below the 25% glucocorticoid percentile, 13/20 (65%) were on GC doses between the 25% and 75% percentiles. The 50% quartile was largely overlapping the medium recommended doses of the British Society of Rheumatology (BSR) and the GiACTA 52-week GC taper (Stone et al, N Engl J Med 2017), but with shorter time spans on doses of 20 mg and above (Figure). On the other hand, the duration on low doses (< 5 mg q.d.) exceeded those of the minimum dose recommendations of the BSR and of the GiACTA 52-week arm (Figure). The respective cumulative prednisolone doses reached in this real-life cohort were 3.74 g for the 25% quartile and 6.22 g for the 75% quartile in the standard dose, and even higher (6.30 g and 8.98 g, respectively) for those starting with high dose GC pulses.
Conclusion: Despite a long-term GC regimen with slow rates of reduction in the low dose range, 44% of the patients relapsed. Only five of these relapses may have been prevented by adhering to the recommended GC regimen, for a still resulting rate of 35% of relapses. Typical cumulative prednisolone doses were slightly lower than those according to the BSR recommendations, because of a probably safe earlier reduction, but still ranged from 3.74 to 8.98 g. These data suggest that GC monotherapy for GCA may be suboptimal.
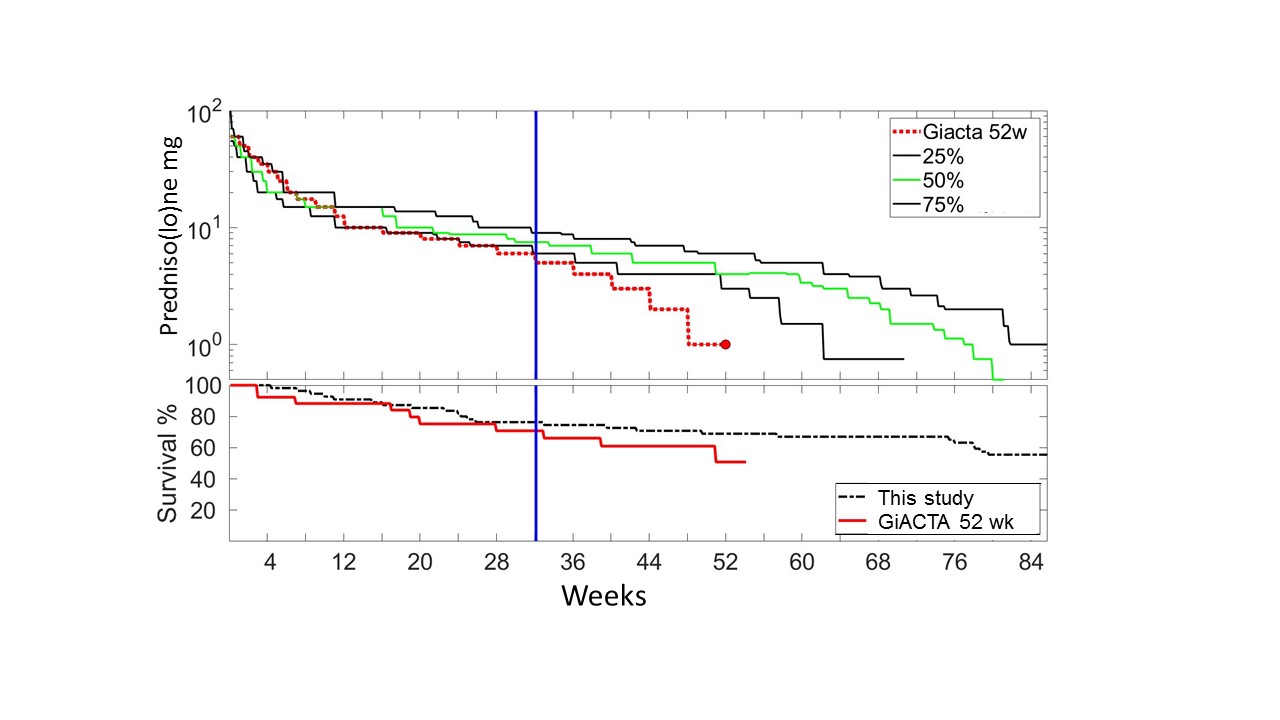 Prednisolone doses and survival without flares of this cohort as compared to the GiACTA 52 week arm. 50% (green), 25% and 75% quartile of the GC doses in the standard dose group of this cohort vs the 52 weeks GC only (pacebo) arm with higher starting dose in the GiACTA trial.
Prednisolone doses and survival without flares of this cohort as compared to the GiACTA 52 week arm. 50% (green), 25% and 75% quartile of the GC doses in the standard dose group of this cohort vs the 52 weeks GC only (pacebo) arm with higher starting dose in the GiACTA trial.
To cite this abstract in AMA style:
Felten L, Leuchten N, Aringer M. In Newly Diagnosed Giant Cell Arteritis in a Real Life Setting Relapses Are Seen in More Than a Third of Patients – and Despite Faster Early Reduction High Cumulative Glucocorticoid Doses Are Reached [abstract]. Arthritis Rheumatol. 2020; 72 (suppl 10). https://acrabstracts.org/abstract/in-newly-diagnosed-giant-cell-arteritis-in-a-real-life-setting-relapses-are-seen-in-more-than-a-third-of-patients-and-despite-faster-early-reduction-high-cumulative-glucocorticoid-doses-are/. Accessed .« Back to ACR Convergence 2020
ACR Meeting Abstracts - https://acrabstracts.org/abstract/in-newly-diagnosed-giant-cell-arteritis-in-a-real-life-setting-relapses-are-seen-in-more-than-a-third-of-patients-and-despite-faster-early-reduction-high-cumulative-glucocorticoid-doses-are/