Session Information
Session Type: Abstract Submissions (ACR)
Background/Purpose: Rheumatoid arthritis (RA) is a chronic inflammatory joint disease which is associated with an increased cardiovascular (CV) risk. Traditional CV risk factors do not fully explain the increased CV risk and prediction of future CV disease in RA by CV risk estimates (Framingham and Reynolds) has shown to be inadequate. The present study investigated whether future CV disease in RA can be accurately predicted by demographic factors, CV risk factors, RA-related factors, CV risk estimates and surrogate markers of CV disease, or a combination of all.
Methods: 10-year incidence rate of CV disease was determined in a prospective cohort of 353 RA-patients. CV risk factors, RA-related factors and surrogate markers of CV disease were assessed at baseline. Predictive models of separate variables or in combinations were created using stepwise backward logistic regression analyses and areas under the curve (AUC) were calculated using receiver operating curves (ROC) analyses.
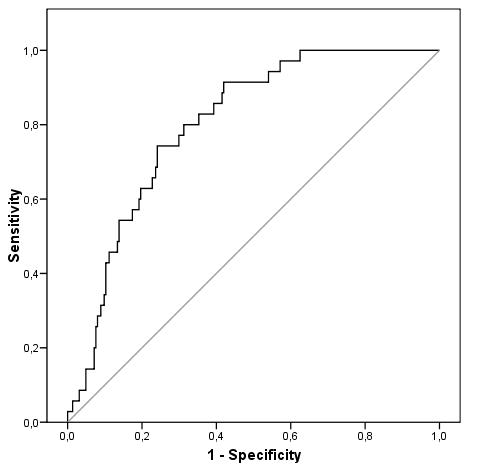
Results: After 10 years, there were 58 events over 2361 patient years of follow-up. CV disease incidence was 16.4%, while 10-year CV risk estimates with SCORE and Framingham underestimated this risk with 5.9% and 13.0%, respectively. From ROC analyses, a model was created which seemed to predict CV disease incidence better than the already available 10-year CV risk estimates (AUC 0.801 vs. 0.712, respectively). For RA patients without prior CV disease, the model consisted of age, gender, use of statins and prednisone, body-mass index, diastolic blood pressure, LDL cholesterol, total cholesterol to HDL-cholesterol ratio, C-reactive protein, HAQ and ESR.
Conclusion: 10-year CV risk estimates did not accurately predict the actual CV risk in a population of RA patients. A combined model of demographic factors, CV risk factors and RA related factors more accurately predicted the actual CV risk. Future studies should corroborate these findings and consider whether modification of pre-existing risk models will improve the CV risk assessment in RA patients.
Table 1. Comparison of incident cardiovascular (CV) disease with 10-year CV risk estimates
|
|
All RA-patients (n=349) |
Prior CV disease excluded (n=295) |
|
Follow-up characteristics |
||
|
Total follow-up, years |
2361 |
2042 |
|
Cases of CV disease, number |
58 |
41 |
|
Incidence rates / 1.000 patient years |
||
|
Total CV disease |
24.6 |
20.1 |
|
CV mortality |
3.4 |
3.4 |
|
Coronary artery disease |
14.4 |
12.2 |
|
Cerebrovascular disease |
6.3 |
4.9 |
|
Peripheral arterial disease |
4.7 |
2.9 |
|
Observed and predicted 10-year CV disease incidence |
||
|
Observed 10-year CV disease incidence, % |
16.4 |
13.9 |
|
Predicted 10-year CV disease risk at baseline according to SCORE-formula, % |
5.9 |
4.9 |
|
Predicted 10-year CV disease risk at baseline according to Framingham-formula, % |
13.0 |
11.0 |
Figure 1. ROC curve for the prediction of incident CV disease using a model consisting of demographical factors, CV risk factors and RA related factors
Disclosure:
A. M. van Sijl,
None;
I. A. M. van den Oever,
None;
M. J. L. Peters,
None;
V. P. van Halm,
None;
A. E. Voskuyl,
None;
Y. M. Smulders,
None;
M. T. Nurmohamed,
None.
« Back to 2012 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-the-accuracy-of-cardiovascular-risk-prediction-in-rheumatoid-arthritis-with-a-new-predictive-model-using-the-10-year-prospective-carre-study/