Session Information
Date: Wednesday, October 24, 2018
Title: 6W019 ACR Abstract: Measures of Healthcare Quality II: QI in SLE, Gout & JIA (2958–2963)
Session Type: ACR Concurrent Abstract Session
Session Time: 11:00AM-12:30PM
Background/Purpose: Juvenile idiopathic arthritis (JIA), the most common pediatric rheumatologic diagnosis, influences many aspects of a child’s life. Although there is no known cure, disease control is often achievable. Early recognition and treatment leads to better disease control that is crucial to prevent chronic pain, irreversible joint damage, and future disability. Clinical Inactive Disease (CID) has been defined and is the accepted outcome measure. In our large pediatric quaternary referral hospital, the number of JIA patients achieving CID was 11% whereas it is reported up to 40% in other centers nationally. Here, we report improvement from 11% to 37% CID within two years by implementing a quality improvement project.
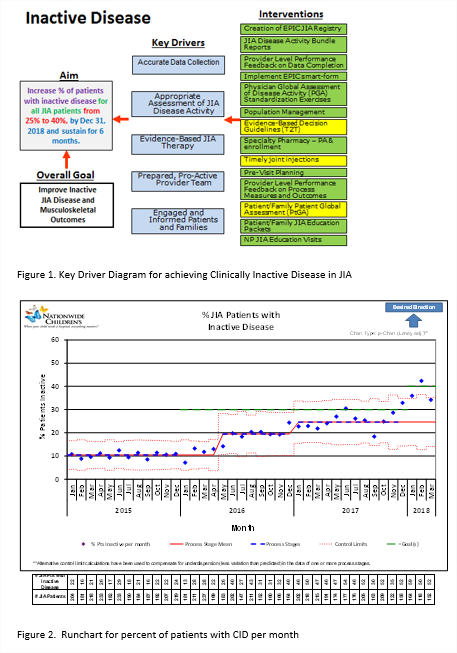
Methods: A key driver diagram (KDD) was used to identify barriers to achieving CID and to develop optimal disease management strategies. The most effective interventions were initially centered around educating parents and patients on disease management, pre-visit planning and provider data entry of disease activity criteria. The physician global assessment (PGA), a subjective score with interprovider variability, was identified as one of the top barriers to inactive disease. In efforts to standardization, PGA scoring exercises were conducted. In addition, providers reviewed currently active patient cases in population management to provide inputs to optimize therapy. These exercises helped standardize disease activity level scoring by allowing providers to challenge each other regarding optimal care of patients. Transparency in provider level feedback surrounding PGA scores and the percentage of patients with inactive disease was shared quarterly with providers. We had multiple other interventions as summarized in KDD (Figure 1).
Results: During the baseline period (Jan 2015-May 2016), only 11% of patients at our center met criteria for CID. After initial interventions, 20% of patients were considered inactive as of June 2016 (p-value <0.001). As population management and PGA exercises took effect, another shift in data occurred in January 2017, resulting in 25% of patients having no disease activity (p-value<0.001). The team has five data point reaching goal, ready for another shift in data (Figure2).
Conclusion: A dedicated QI project, focusing on multiple interventions, improved the disease activity level of patients with JIA. It is expected that as the team continues with these exercises and proceeds with next steps, the percentage of patients with inactive disease will continue to rise.
To cite this abstract in AMA style:
Yildirim-Toruner C, AlAhmed O, Barbar-Smiley F, Jones K, Kohlheim M, Lemle S, MacDonald D, Mulvihill E, Oberle E, Sarkissian A, Sivaraman V, Thomas B, Wise K, Ardoin SP. Improving Clinically Inactive Disease in Patients with Juvenile Idiopathic Arthritis- a Quaternary Center Experience [abstract]. Arthritis Rheumatol. 2018; 70 (suppl 9). https://acrabstracts.org/abstract/improving-clinically-inactive-disease-in-patients-with-juvenile-idiopathic-arthritis-a-quaternary-center-experience/. Accessed .« Back to 2018 ACR/ARHP Annual Meeting
ACR Meeting Abstracts - https://acrabstracts.org/abstract/improving-clinically-inactive-disease-in-patients-with-juvenile-idiopathic-arthritis-a-quaternary-center-experience/